

Global, regional, and national burden of hepatitis B, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019
- PMID: 35738290
- PMCID: PMC9349325
- DOI: 10.1016/S2468-1253(22)00124-8
Global, regional, and national burden of hepatitis B, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019
Abstract
Background: Combating viral hepatitis is part of the UN Sustainable Development Goals (SDGs), and WHO has put forth hepatitis B elimination targets in its Global Health Sector Strategy on Viral Hepatitis (WHO-GHSS) and Interim Guidance for Country Validation of Viral Hepatitis Elimination (WHO Interim Guidance). We estimated the global, regional, and national prevalence of hepatitis B virus (HBV), as well as mortality and disability-adjusted life-years (DALYs) due to HBV, as part of the Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019. This included estimates for 194 WHO member states, for which we compared our estimates to WHO elimination targets.
Methods: The primary data sources were population-based serosurveys, claims and hospital discharges, cancer registries, vital registration systems, and published case series. We estimated chronic HBV infection and the burden of HBV-related diseases, defined as an aggregate of cirrhosis due to hepatitis B, liver cancer due to hepatitis B, and acute hepatitis B. We used DisMod-MR 2.1, a Bayesian mixed-effects meta-regression tool, to estimate the prevalence of chronic HBV infection, cirrhosis, and aetiological proportions of cirrhosis. We used mortality-to-incidence ratios modelled with spatiotemporal Gaussian process regression to estimate the incidence of liver cancer. We used the Cause of Death Ensemble modelling (CODEm) model, a tool that selects models and covariates on the basis of out-of-sample performance, to estimate mortality due to cirrhosis, liver cancer, and acute hepatitis B.
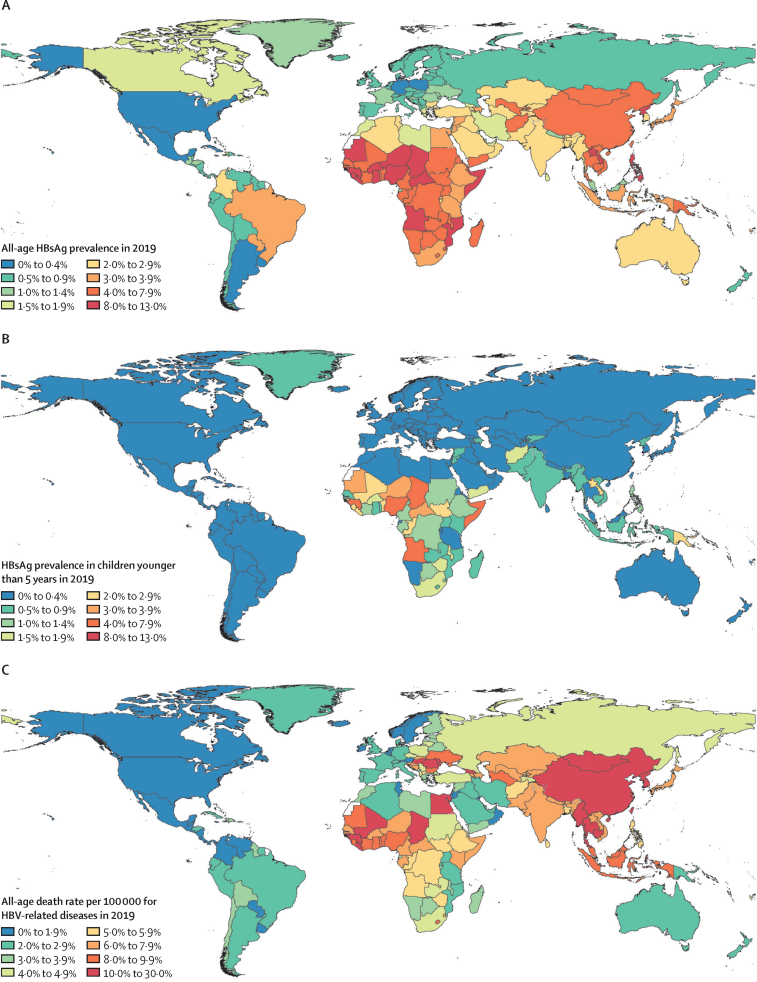
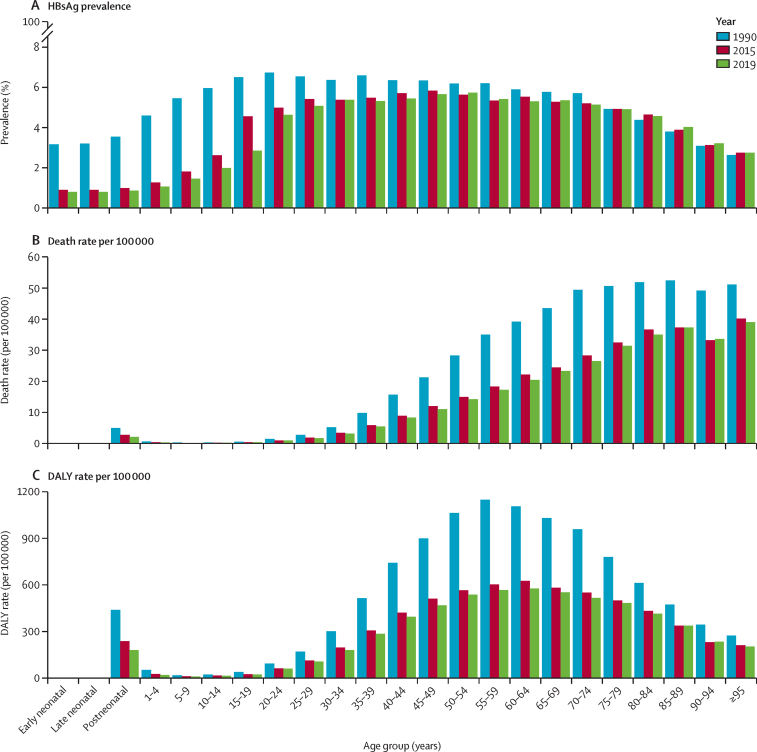
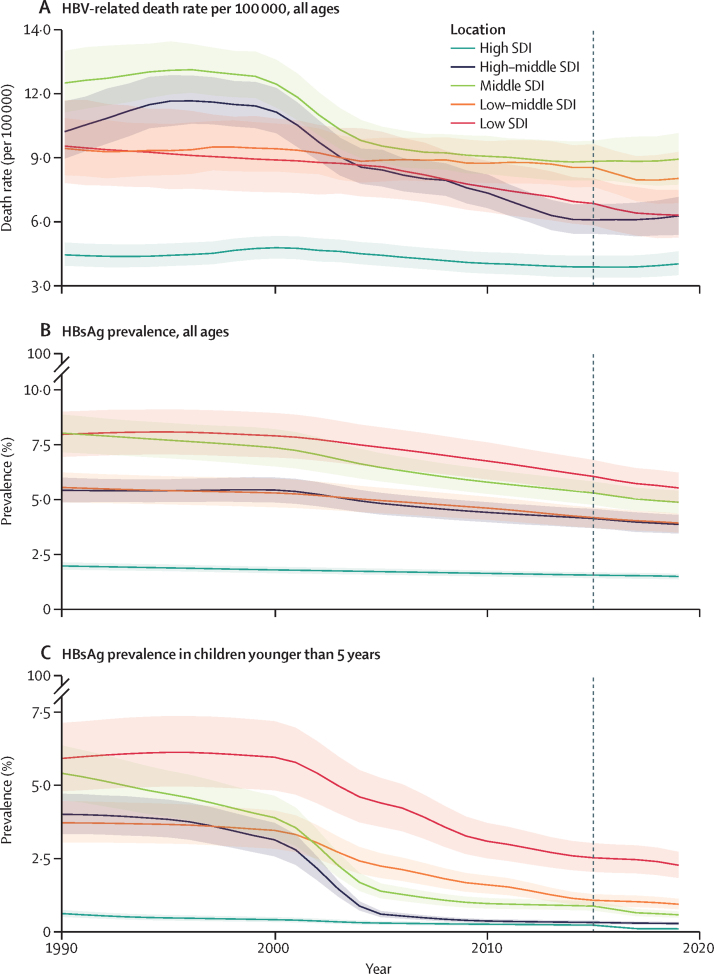
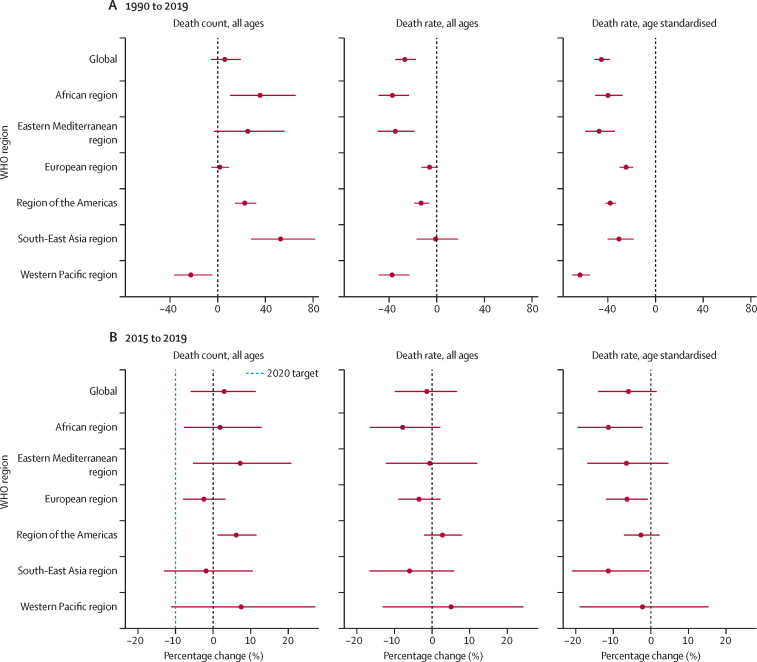
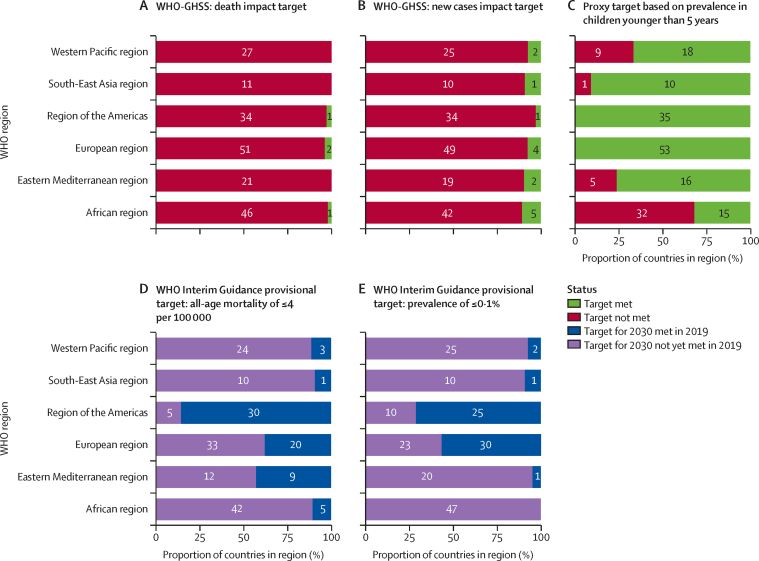
Findings: In 2019, the estimated global, all-age prevalence of chronic HBV infection was 4·1% (95% uncertainty interval [UI] 3·7 to 4·5), corresponding to 316 million (284 to 351) infected people. There was a 31·3% (29·0 to 33·9) decline in all-age prevalence between 1990 and 2019, with a more marked decline of 76·8% (76·2 to 77·5) in prevalence in children younger than 5 years. HBV-related diseases resulted in 555 000 global deaths (487 000 to 630 000) in 2019. The number of HBV-related deaths increased between 1990 and 2019 (by 5·9% [-5·6 to 19·2]) and between 2015 and 2019 (by 2·9% [-5·9 to 11·3]). By contrast, all-age and age-standardised death rates due to HBV-related diseases decreased during these periods. We compared estimates for 2019 in 194 WHO locations to WHO-GHSS 2020 targets, and found that four countries achieved a 10% reduction in deaths, 15 countries achieved a 30% reduction in new cases, and 147 countries achieved a 1% prevalence in children younger than 5 years. As of 2019, 68 of 194 countries had already achieved the 2030 target proposed in WHO Interim Guidance of an all-age HBV-related death rate of four per 100 000.
Interpretation: The prevalence of chronic HBV infection declined over time, particularly in children younger than 5 years, since the introduction of hepatitis B vaccination. HBV-related death rates also decreased, but HBV-related death counts increased as a result of population growth, ageing, and cohort effects. By 2019, many countries had met the interim seroprevalence target for children younger than 5 years, but few countries had met the WHO-GHSS interim targets for deaths and new cases. Progress according to all indicators must be accelerated to meet 2030 targets, and there are marked disparities in burden and progress across the world. HBV interventions, such as vaccination, testing, and treatment, must be strategically supported and scaled up to achieve elimination.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests S Afzal reports participation on a data safety monitoring board or advisory board on the Corona Expert Advisory Group and Infectious Diseases Expert Advisory Group; leadership or fiduciary roles in other board, society, committee or advocacy groups, paid or unpaid, as a Fellow of the Faculty of Public Health (UK), and as the Dean of Public Health and Preventive Medicine, and the Chairperson of Medicine at the King Edward Medical University (Lahore, Pakistan); all outside the submitted work. R Ancuceanu reports consulting fees from AbbVie; payment or honoraria for lectures, presentations, speakers' bureau, manuscript writing, or educational events from from AbbVie, Sandoz, and B Braun; all outside the submitted work. M Ausloos reports grants from Romanian National Authority for Scientific Research and Innovation (CNDS-UEFISCDI; project number PN-III-P4-ID-PCCF-2016-0084 Oct 2018–Sep 2022), outside the submitted work. X Dai reports support for the present manuscript from the University of Washington (Seattle, WA, USA), through their employment at IHME. T M Drake reports grant funding from Aligod Therapeutics for research into primary liver cancer, outside the submitted work. C Herteliu reports grants from CNDS-UEFISCDI (project numbers PN-III-P4-ID-PCCF-2016-0084 Oct 2018–Sept 2022 and PN-III-P2–2.1-SOL-2020-2-0351 June 2020–Oct 2020), from the Romanian Ministry of Research Innovation and Digitalization (project number ID-585-CTR-42-PFE-2021 Jan 2022–June 2023), and from the Ministry of Labour and Social Justice, Romania (project number 30/PSCD/2018 Sept 2018–June 2019), outside the submitted work. L Hiebert reports grants or contracts through the Task Force for Global Health, which receives funds for the general support of the Coalition for Global Hepatitis Elimination from Abbott, Gilead, AbbVie, Merck, Siemens, Cepheid, Roche, Pharco, Zydus-Cadila, and governmental agencies and philanthropic organisations; outside the submitted work. N E Ismail reports leadership or fiduciary roles in other board, society, committee or advocacy groups, unpaid, as a council member of the Malaysian Academy of Pharmacy, outside the submitted work. I M Karaye reports support for attending meetings or travel, or both, from Hofstra University for the Natural Hazards meeting and American College of Epidemiology Conference, outside the submitted work. J V Lazarus reports grants and consulting fees from AbbVie, Gilead Sciences, and MSD; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from AbbVie, Gilead, Sciences, Intercept, Jannsen, and MSD; leadership or fiduciary roles in other board, society, committee or advocacy groups, unpaid, with the EASL international Liver Foundation; all outside the submitted work. J A Loureiro reports support for the present manuscript from Fundaçã o para a Ciência e Técnologia (FCT) under the Scientific Employment Stimulus (CEECINST/00049/2018). P C Matthews reports support for the present manuscript from the Welcome Trust through the Intermediate Clinical Fellowship (grant Ref 110110/Z/15/Z); grants or contracts from GlaxoSmithKline as a contribution to their PhD stipend; and royalties from Oxford University Press for the publication of a medical textbook; all outside the submitted work. O O Odukoya reports support for the present manuscript from the Fogarty International Center of the National Institutes of Health under the Award Number K43TW010704. M J Postma reports stock or stock options in HealthEcore and PAG, outside the submitted work. A Pana reports grants from CNDS-UEFISCDI (project numbers PN-III-P4-ID-PCCF-2016–0084 Oct 2018–Sep 2022 and PN-III-P2–2·1-SOL-2020–2-0351 June 2020–Oct 2020), outside the submitted work. J Sanabria reports grants for contracts from Marshall University School of Medicine and Joan Edwards Comprehensive Cancer Center (Huntington, WV, USA); patents planned, issued, or pending for pNaKtide for the treatment of hepatocellular carcinoma related to NASH and NASH; participation on a data safety monitoring board or advisory board with the Department of Surgery, Marshall University, as a quality assessment and assurance officer; leadership or fiduciary roles in other board, society, committee or advocacy groups, and unpaid roles with several national and international surgical societies; all outside the submitted work. J A Singh reports consulting fees from Crealta/Horizon, Medisys, Fidia, PK Med, Two labs, Adept Field Solutions, Clinical Care options, Clearview Healthcare Partners, Putnam Associates, Focus Forward, Navigant Consulting, Spherix, MedIQ, Jupiter Life, UBM, Trio Health, Medscape, WebMD, Practice Point Communications, the US National Institutes of Health, and the American College of Rheumatology; payment or honoraria for participating in the speakers bureau for Simply Speaking; support for attending meetings or travel, or both, from the steering committee of OMERACT, to attend their meeting every 2 years; participation on a data safety monitoring board or advisory board as an unpaid member of the US Food and Drug Administration (FDA) Arthritis Advisory Committee; leadership or fiduciary roles in other board, society, committee or advocacy groups, paid or unpaid, as a member of the steering committee of OMERACT, an international organisation that develops measures for clinical trials and receives arms' length funding from 12 pharmaceutical companies, with the Veterans Affairs Rheumatology Field Advisory Committee as Chair, and with the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis as a director and editor; stock or stock options in TPT Global Tech, Vaxart Pharmaceuticals, Atyu Biopharma, Adaptimmune Therapeutics, GeoVax Labs, Pieris Pharmaceuticals, Enzolytics, Series Therapeutics, Tonix Pharmaceuticals, and Charlotte's Web Holdings; and previously owned stock options in Amarin, Viking, and Moderna; all outside the submitted work. J W Ward reports grants or contracts through The Task Force for Global Health, which receives funds for the general support of the Coalition for Global Hepatitis Elimination from Abbott, Gilead, AbbVie, Merck, Siemens, Cepheid, Roche, Pharco, Zydus-Cadila, governmental agencies and philanthropic organisations; membership on an advisory board, unpaid, with the international Coalition to Eliminate HBV, and membership on an advisory committee, unpaid, for the Longevity Project for HCV at the University of Liverpool (UK); all outside the submitted work.
Figures
References
-
- WHO Hepatitis B vaccines: WHO position paper—recommendations. Vaccine. 2010;28:589–590. - PubMed
-
- Perz JF, Armstrong GL, Farrington LA, Hutin YJF, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol. 2006;45:529–538. - PubMed
