

The influence of ambulance offload time on 30-day risks of death and re-presentation for patients with chest pain
- PMID: 35738570
- PMCID: PMC9545565
- DOI: 10.5694/mja2.51613
The influence of ambulance offload time on 30-day risks of death and re-presentation for patients with chest pain
Abstract
Objective: To assess whether ambulance offload time influences the risks of death or ambulance re-attendance within 30 days of initial emergency department (ED) presentations by adults with non-traumatic chest pain.
Design, setting: Population-based observational cohort study of consecutive presentations by adults with non-traumatic chest pain transported by ambulance to Victorian EDs, 1 January 2015 - 30 June 2019.
Participants: Adults (18 years or older) with non-traumatic chest pain, excluding patients with ST elevation myocardial infarction (pre-hospital electrocardiography) and those who were transferred between hospitals or not transported to hospital (eg, cardiac arrest or death prior to transport).
Main outcome measures: Primary outcome: 30-day all-cause mortality (Victorian Death Index data).
Secondary outcome: Transport by ambulance with chest pain to ED within 30 days of initial ED presentation.
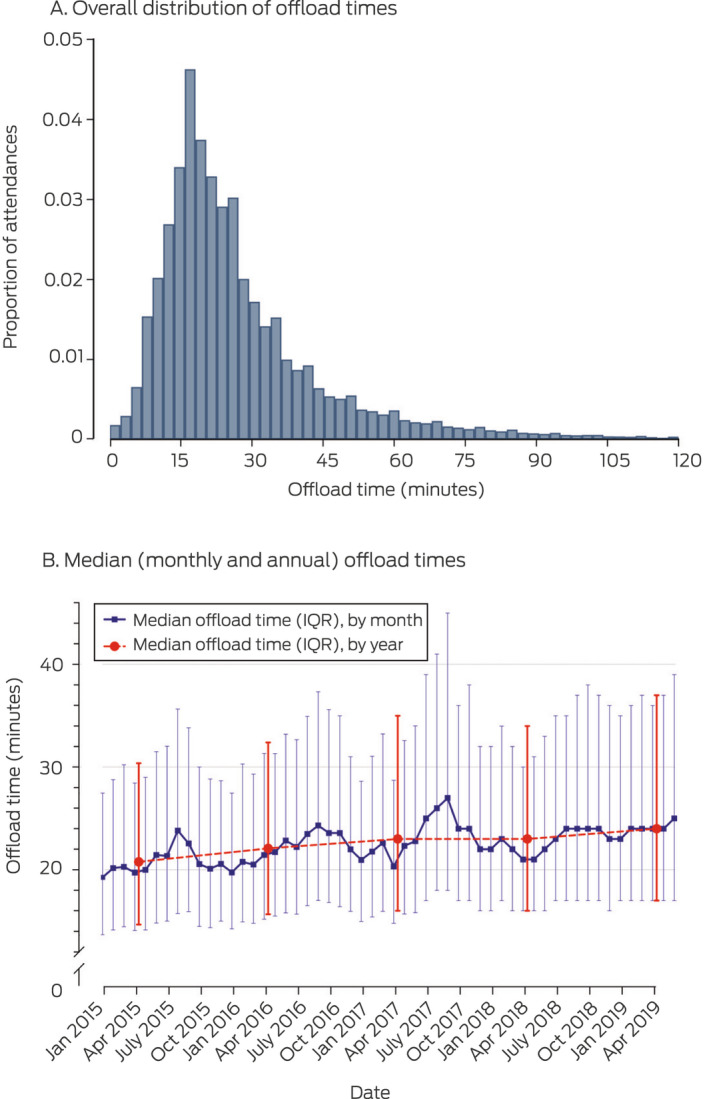
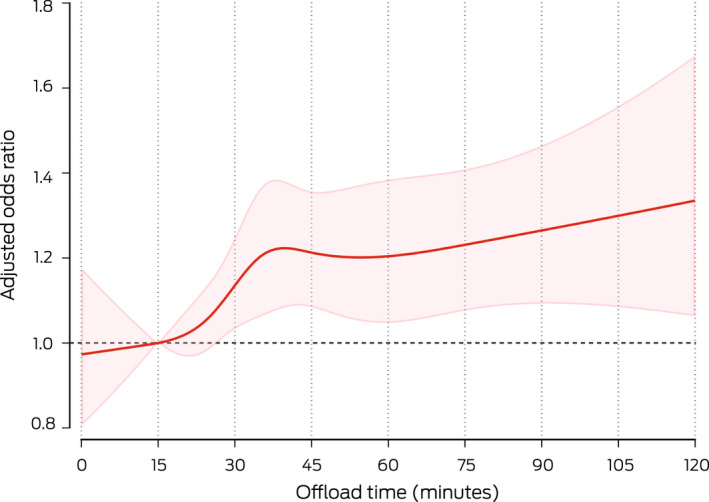
Results: We included 213 544 people with chest pain transported by ambulance to EDs (mean age, 62 [SD, 18] years; 109 027 women [51%]). The median offload time increased from 21 (IQR, 15-30) minutes in 2015 to 24 (IQR, 17-37) minutes during the first half of 2019. Three offload time tertiles were defined to include approximately equal patient numbers: tertile 1 (0-17 minutes), tertile 2 (18-28 minutes), and tertile 3 (more than 28 minutes). In multivariable models, 30-day risk of death was greater for patients in tertile 3 than those in tertile 1 (adjusted rates, 1.57% v 1.29%; adjusted risk difference, 0.28 [95% CI, 0.16-0.42] percentage points), as was that of a second ambulance attendance with chest pain (adjusted rates, 9.03% v 8.15%; adjusted risk difference, 0.87 [95% CI, 0.57-1.18] percentage points).
Conclusions: Longer ambulance offload times are associated with greater 30-day risks of death and ambulance re-attendance for people presenting to EDs with chest pain. Improving the speed of ambulance-to-ED transfers is urgently required.
Keywords: Acute coronary syndrome; Emergency services, medical; Public health; Transportation of patients; Treatment outcome.
© 2022 The Authors. Medical Journal of Australia published by John Wiley & Sons Australia, Ltd on behalf of AMPCo Pty Ltd.
Conflict of interest statement
No relevant disclosures.
Figures
Comment in
-
Ambulance ramping and patients with cardiac-type symptoms: understanding the unloading queue.Med J Aust. 2022 Sep 5;217(5):238-239. doi: 10.5694/mja2.51677. Epub 2022 Aug 5. Med J Aust. 2022. PMID: 35929413 No abstract available.
-
The influence of ambulance offload time on 30-day risks of death and re-presentation for patients with chest pain.Med J Aust. 2023 Feb 20;218(3):142. doi: 10.5694/mja2.51812. Epub 2022 Dec 9. Med J Aust. 2023. PMID: 36494080 No abstract available.
-
The influence of ambulance offload time on 30-day risks of death and re-presentation for patients with chest pain.Med J Aust. 2023 Feb 20;218(3):142. doi: 10.5694/mja2.51806. Epub 2022 Dec 9. Med J Aust. 2023. PMID: 36494082 No abstract available.
Similar articles
-
Variation in Health Care Processes, Quality and Outcomes According to Day and Time of Chest Pain Presentation via Ambulance.Heart Lung Circ. 2023 Jun;32(6):709-718. doi: 10.1016/j.hlc.2023.03.013. Epub 2023 Apr 24. Heart Lung Circ. 2023. PMID: 37100698
-
Assessing sensitivity and specificity of the Manchester Triage System in the evaluation of acute coronary syndrome in adult patients in emergency care: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Nov;13(11):64-73. doi: 10.11124/jbisrir-2015-2213. JBI Database System Rev Implement Rep. 2015. PMID: 26657465
-
Effect of a mass media campaign on ambulance use for chest pain.Med J Aust. 2017 Jan 16;206(1):30-35. doi: 10.5694/mja16.00341. Med J Aust. 2017. PMID: 28076734
-
Context-independent identification of myocardial ischemia in the prehospital ECG of chest pain patients.J Electrocardiol. 2024 Jan-Feb;82:34-41. doi: 10.1016/j.jelectrocard.2023.10.009. Epub 2023 Nov 7. J Electrocardiol. 2024. PMID: 38006762 Review.
-
Ambulance diversion and emergency department offload delay: resource document for the National Association of EMS Physicians position statement.Prehosp Emerg Care. 2011 Oct-Dec;15(4):555-61. doi: 10.3109/10903127.2011.608871. Prehosp Emerg Care. 2011. PMID: 21870947 Review.
Cited by
-
Patterns in California Ambulance Patient Offload Times by Local Emergency Medical Services Agency.JAMA Netw Open. 2024 Dec 2;7(12):e2451022. doi: 10.1001/jamanetworkopen.2024.51022. JAMA Netw Open. 2024. PMID: 39680409 Free PMC article.
-
The Safety INdEx of Prehospital On Scene Triage (SINEPOST) study: The development and validation of a risk prediction model to support ambulance clinical transport decisions on-scene.PLoS One. 2022 Nov 16;17(11):e0276515. doi: 10.1371/journal.pone.0276515. eCollection 2022. PLoS One. 2022. PMID: 36383548 Free PMC article.
-
Racial and Socioeconomic Disparities in California Ambulance Patient Offload Times.JAMA Netw Open. 2025 May 1;8(5):e2510325. doi: 10.1001/jamanetworkopen.2025.10325. JAMA Netw Open. 2025. PMID: 40372755 Free PMC article.
-
Ambulance offload performance, patient characteristics and disposition for patients offloaded to different areas of the emergency department.Emerg Med Australas. 2025 Feb;37(1):e14517. doi: 10.1111/1742-6723.14517. Epub 2024 Oct 10. Emerg Med Australas. 2025. PMID: 39389920 Free PMC article.
References
-
- House J. What’s causing England’s A&E crisis? Lancet 2013; 382: 195‐196. - PubMed
-
- Kingswell C, Shaban RZ, Crilly J. Concepts, antecedents and consequences of ambulance ramping in the emergency department: a scoping review. Australas Emerg Nurs J 2017; 20: 153‐160. - PubMed
-
- Li M, Vanberkel P, Carter AJE. A review on ambulance offload delay literature. Health Care Manag Sci 2019; 22: 658‐675. - PubMed
-
- Stewart D, Lang E, Wang D, Innes G. Are emergency medical services offload delay patients at increased risk of adverse outcomes? CJEM 2019; 21: 505‐512. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
