

Cost and cost effectiveness of reactive case detection (RACD), reactive focal mass drug administration (rfMDA) and reactive focal vector control (RAVC) to reduce malaria in the low endemic setting of Namibia: an analysis alongside a 2×2 factorial design cluster randomised controlled trial
- PMID: 35738650
- PMCID: PMC9226870
- DOI: 10.1136/bmjopen-2021-049050
Cost and cost effectiveness of reactive case detection (RACD), reactive focal mass drug administration (rfMDA) and reactive focal vector control (RAVC) to reduce malaria in the low endemic setting of Namibia: an analysis alongside a 2×2 factorial design cluster randomised controlled trial
Abstract
Objectives: To estimate the cost and cost effectiveness of reactive case detection (RACD), reactive focal mass drug administration (rfMDA) and reactive focal vector control (RAVC) to reduce malaria in a low endemic setting.
Setting: The study was part of a 2×2 factorial design cluster randomised controlled trial within the catchment area of 11 primary health facilities in Zambezi, Namibia.
Participants: Cost and outcome data were collected from the trial, which included 8948 community members that received interventions due to their residence within 500 m of malaria index cases.
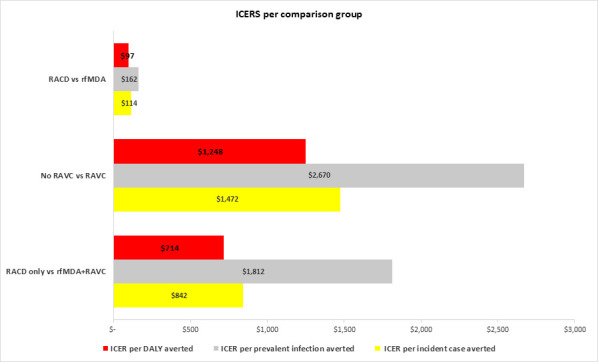
Outcome measures: The primary outcome was incremental cost effectiveness ratio (ICER) per in incident case averted. ICER per prevalent case and per disability-adjusted life years (DALY) averted were secondary outcomes, as were per unit interventions costs and personnel time. Outcomes were compared as: (1) rfMDA versus RACD, (2) RAVC versus no RAVC and (3) rfMDA+RAVC versus RACD only.
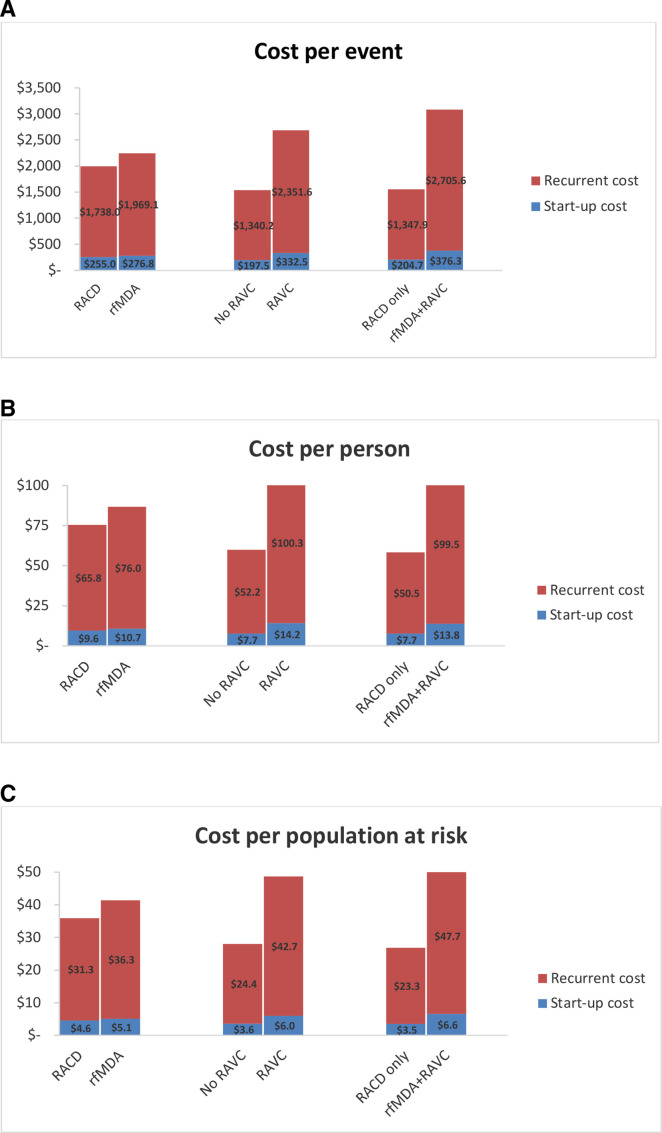
Results: rfMDA cost 1.1× more than RACD, and RAVC cost 1.7× more than no RAVC. Relative to RACD only, the cost of rfMDA+RAVC was double ($3082 vs $1553 per event). The ICERs for rfMDA versus RACD, RAVC versus no RAVC and rfMDA+RAVC versus RACD only were $114, $1472 and $842, per incident case averted, respectively. Using prevalent infections and DALYs as outcomes, trends were similar. The median personnel time to implement rfMDA was 20% lower than for RACD (30 vs 38 min per person). The median personnel time for RAVC was 34 min per structure sprayed.
Conclusion: Implemented alone or in combination, rfMDA and RAVC were cost effective in reducing malaria incidence and prevalence despite higher implementation costs in the intervention compared with control arms. Compared with RACD, rfMDA was time saving. Cost and time requirements for the combined intervention could be decreased by implementing rfMDA and RAVC simultaneously by a single team.
Trial registration number: NCT02610400; Post-results.
Keywords: EPIDEMIOLOGY; HEALTH ECONOMICS; Health policy; Public health.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures


Similar articles
-
Effectiveness of reactive focal mass drug administration and reactive focal vector control to reduce malaria transmission in the low malaria-endemic setting of Namibia: a cluster-randomised controlled, open-label, two-by-two factorial design trial.Lancet. 2020 Apr 25;395(10233):1361-1373. doi: 10.1016/S0140-6736(20)30470-0. Lancet. 2020. PMID: 32334702 Free PMC article. Clinical Trial.
-
Study protocol for a cluster randomised controlled factorial design trial to assess the effectiveness and feasibility of reactive focal mass drug administration and vector control to reduce malaria transmission in the low endemic setting of Namibia.BMJ Open. 2018 Jan 27;8(1):e019294. doi: 10.1136/bmjopen-2017-019294. BMJ Open. 2018. PMID: 29374672 Free PMC article. Clinical Trial.
-
Community acceptance of reactive focal mass drug administration and reactive focal vector control using indoor residual spraying, a mixed-methods study in Zambezi region, Namibia.Malar J. 2021 Mar 22;20(1):162. doi: 10.1186/s12936-021-03679-1. Malar J. 2021. PMID: 33752673 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Reactive Case Detection (RACD) and foci investigation strategies in malaria control and elimination: a review.Malar J. 2020 Nov 10;19(1):401. doi: 10.1186/s12936-020-03478-0. Malar J. 2020. PMID: 33172462 Free PMC article. Review.
Cited by
-
Advancing malaria reactive case detection in a Zambia-like setting: A modeling study.PLOS Glob Public Health. 2025 Feb 20;5(2):e0004288. doi: 10.1371/journal.pgph.0004288. eCollection 2025. PLOS Glob Public Health. 2025. PMID: 39977420 Free PMC article.
-
Extension of efficacy range for targeted malaria-elimination interventions due to spillover effects.Nat Med. 2024 Oct;30(10):2813-2820. doi: 10.1038/s41591-024-03134-z. Epub 2024 Jul 4. Nat Med. 2024. PMID: 38965434 Free PMC article. Clinical Trial.
-
Effectiveness and Efficacy of Long-Lasting Insecticidal Nets for Malaria Control in Africa: Systematic Review and Meta-Analysis of Randomized Controlled Trials.Int J Environ Res Public Health. 2025 Jun 30;22(7):1045. doi: 10.3390/ijerph22071045. Int J Environ Res Public Health. 2025. PMID: 40724110 Free PMC article. Review.
-
Testing and treatment for malaria elimination: a systematic review.Malar J. 2023 Sep 3;22(1):254. doi: 10.1186/s12936-023-04670-8. Malar J. 2023. PMID: 37661286 Free PMC article.
-
How Real-Time Case-Based Malaria Surveillance Helps Zanzibar Get a Step Closer to Malaria Elimination: Description of Operational Platform and Resources.Glob Health Sci Pract. 2023 Oct 30;11(5):e2200522. doi: 10.9745/GHSP-D-22-00522. Print 2023 Oct 30. Glob Health Sci Pract. 2023. PMID: 37903584 Free PMC article.
References
-
- WHO . World malaria report 2019, 2019.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical