

New insights from non-invasive imaging: from prospection of skin photodamages to training with mobile application
- PMID: 35738810
- PMCID: PMC9328152
- DOI: 10.1111/jdv.18197
New insights from non-invasive imaging: from prospection of skin photodamages to training with mobile application
Abstract
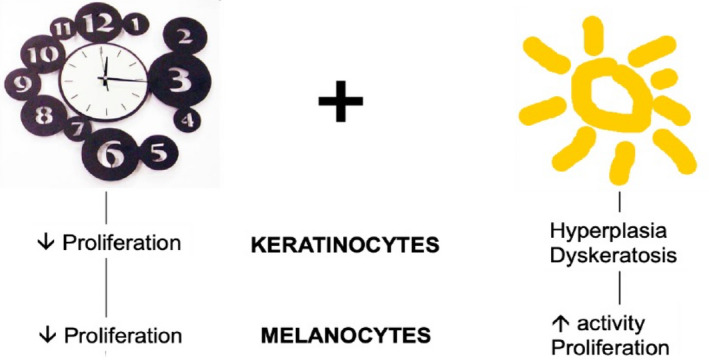
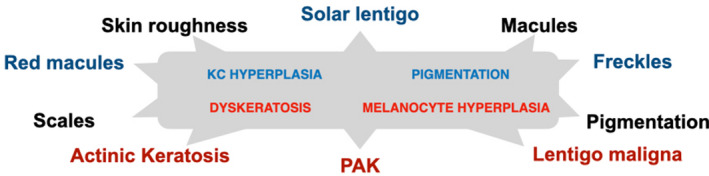
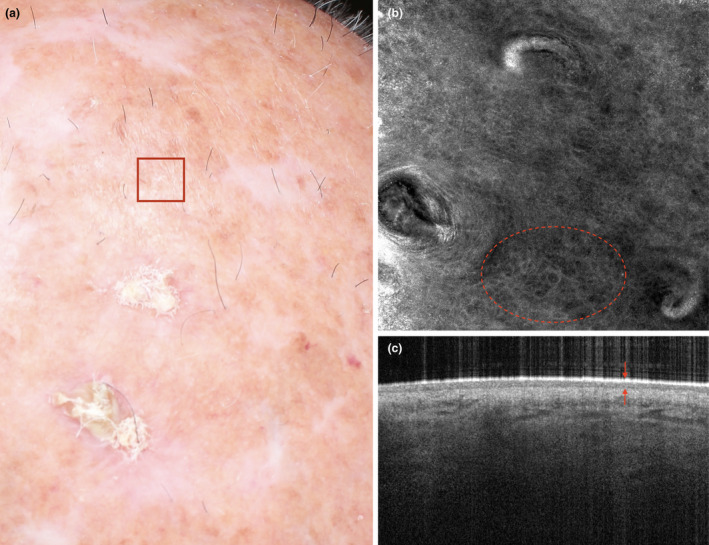
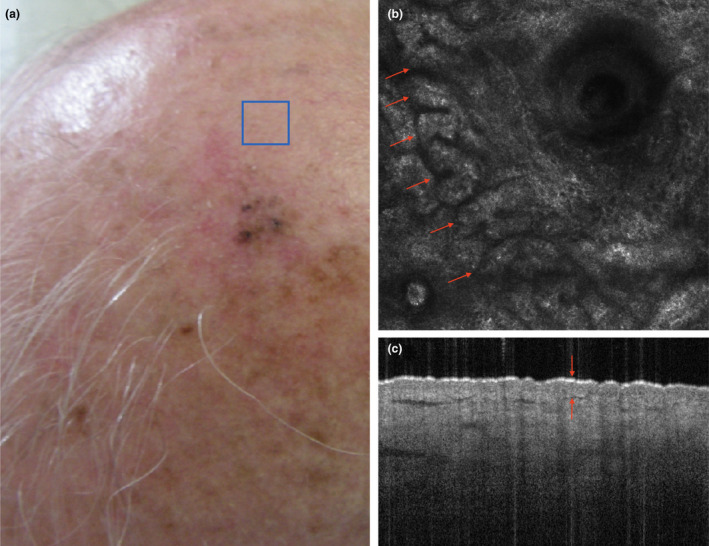
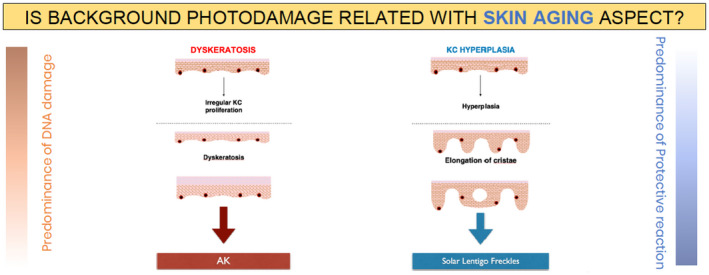
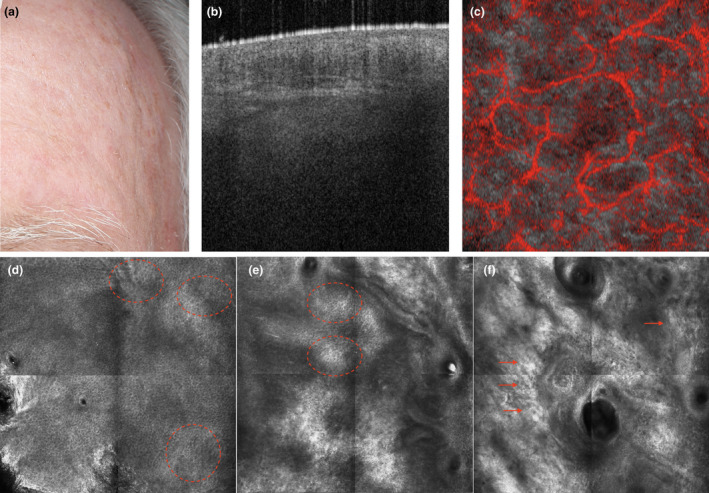
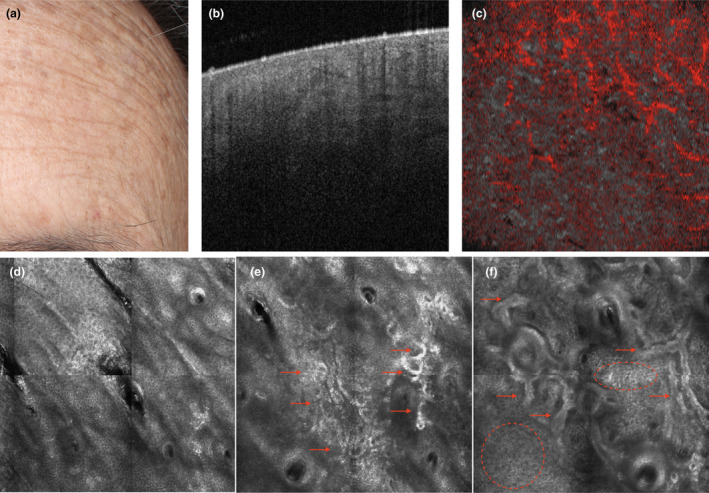
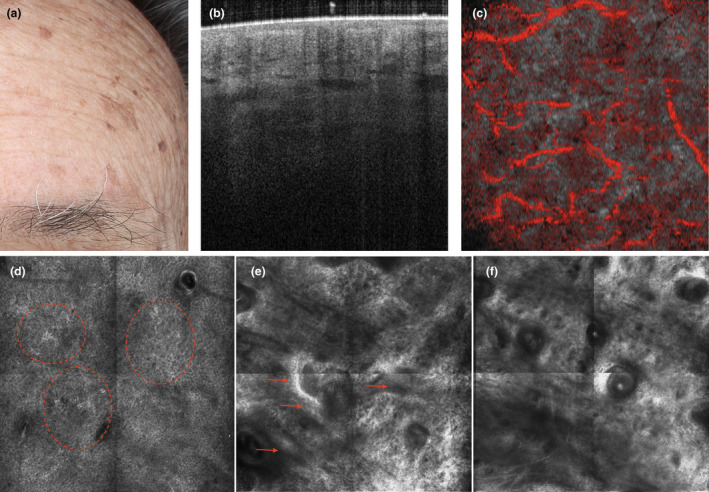
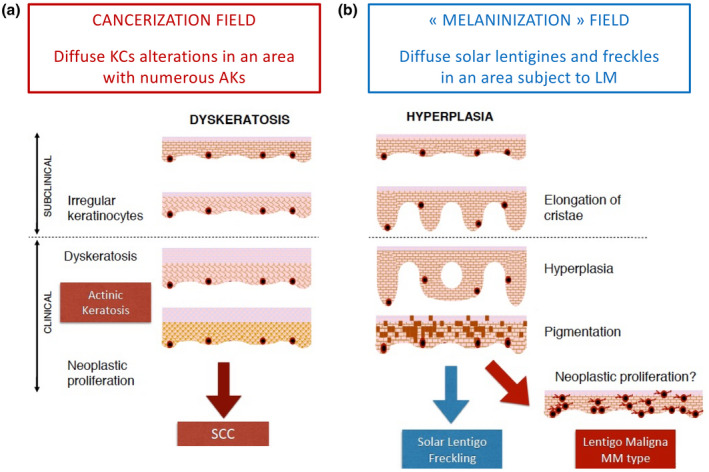
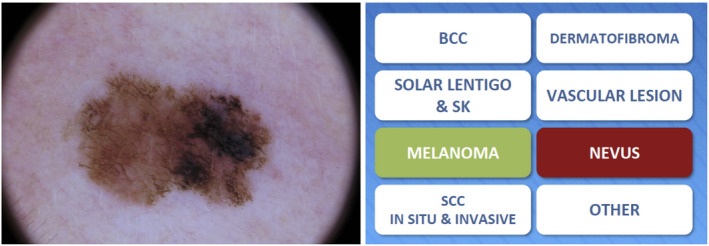
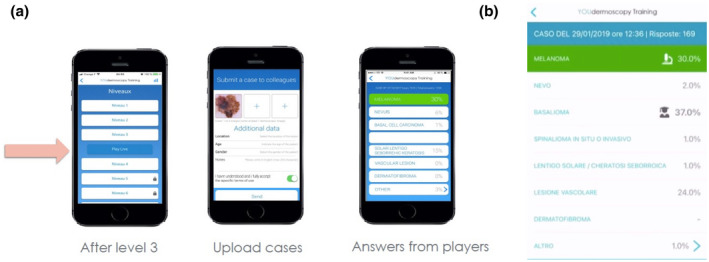
The incidence of non-melanoma skin cancer is on the rise and melanoma is among the most common cancers in the United States. Establishing an early diagnosis is essential for improving the prognosis of patients with skin cancer. High-resolution non-invasive imaging techniques may represent key tools for helping to identify and monitor early signs of skin cancer in seemingly healthy skin. Cumulative lifetime sun exposure leads to photoaging and photocarcinogenenis and the reaction of the skin to this solar-induced damage is balanced between the DNA repair and photoprotection defence mechanisms of melanocytes and keratinocytes. In the first part of this article we provide an overview of these defence mechanisms and of the photoaging process, and discuss how non-invasive imaging can be used to evaluate these changes. We then propose a model in which skin aging manifestations can be classified according to subject-specific sun-damage reaction profiles observed by reflectance confocal microscopy (RCM) and optical coherence tomography (OCT). These photoaging profiles include an atrophic phenotype characterized by actinic keratosis, and a hypertrophic phenotype characterized by hyperplastic pigmented skin. According to our model, these phenotypes may be predictive of predispositions to different types of skin cancer: squamous cell carcinoma for the atrophic phenotype and lentigo maligna and freckles for the hypertrophic phenotype. In addition to RCM and OCT, dermoscopy is another non-invasive technique that has improved the diagnosis of skin cancer. In the second part of this article, we describe how the YouDermoscopy™ application can improve skills and thus enhance the dermoscopic recognition of sun-induced skin tumours, and then show how this training tool enables its users to collaborate with dermatologists worldwide to obtain second opinions for the diagnosis of ambiguous lesions. Altogether, RCM, OCT and dermoscopy are valuable tools that can contribute significantly to improving the early diagnosis of precancerous and cancerous lesions.
Keywords: actinic keratosis; confocal microscopy; dermoscopy; diagnosis; melanoma.
© 2022 The Authors. Journal of the European Academy of Dermatology and Venereology published by John Wiley & Sons Ltd on behalf of European Academy of Dermatology and Venereology.
Figures
Similar articles
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
-
Reflectance confocal microscopy correlates of dermoscopic patterns of facial lesions help to discriminate lentigo maligna from pigmented nonmelanocytic macules.Br J Dermatol. 2015 Jul;173(1):128-33. doi: 10.1111/bjd.13546. Epub 2015 Mar 31. Br J Dermatol. 2015. PMID: 25413382
-
The combination of dermoscopy and reflectance confocal microscopy increases the diagnostic confidence of amelanotic/hypomelanotic lentigo maligna.J Dermatol. 2024 May;51(5):714-718. doi: 10.1111/1346-8138.17075. Epub 2024 Jan 13. J Dermatol. 2024. PMID: 38217366 Free PMC article.
-
Reflectance confocal microscopy to diagnose malignant melanoma and lentigo maligna in the UK: a single-centre prospective observational trial.Br J Dermatol. 2024 Dec 23;192(1):27-35. doi: 10.1093/bjd/ljae354. Br J Dermatol. 2024. PMID: 39255055
-
Reflectance confocal microscopy in the diagnosis of pigmented macules of the face: differential diagnosis and margin definition.Photochem Photobiol Sci. 2019 May 15;18(5):963-969. doi: 10.1039/c8pp00525g. Photochem Photobiol Sci. 2019. PMID: 30938378 Review.
Cited by
-
Dysregulation of autophagy during photoaging reduce oxidative stress and inflammatory damage caused by UV.Front Pharmacol. 2025 May 12;16:1562845. doi: 10.3389/fphar.2025.1562845. eCollection 2025. Front Pharmacol. 2025. PMID: 40421222 Free PMC article. Review.
-
Noninvasive Technologies for the Diagnosis of Squamous Cell Carcinoma: A Systematic Review and Meta-Analysis.JID Innov. 2024 Jul 20;4(6):100303. doi: 10.1016/j.xjidi.2024.100303. eCollection 2024 Nov. JID Innov. 2024. PMID: 39263563 Free PMC article. Review.
-
Age-Related Dysfunction in Balance: A Comprehensive Review of Causes, Consequences, and Interventions.Aging Dis. 2024 Jan 24;16(2):714-737. doi: 10.14336/AD.2024.0124-1. Aging Dis. 2024. PMID: 38607735 Free PMC article. Review.
-
Mechanisms and Therapeutic Roles of Medicinal Plants in Skin Photoaging.Clin Cosmet Investig Dermatol. 2025 Jul 11;18:1709-1726. doi: 10.2147/CCID.S538326. eCollection 2025. Clin Cosmet Investig Dermatol. 2025. PMID: 40666164 Free PMC article. Review.
-
Current advance of nanotechnology in diagnosis and treatment for malignant tumors.Signal Transduct Target Ther. 2024 Aug 12;9(1):200. doi: 10.1038/s41392-024-01889-y. Signal Transduct Target Ther. 2024. PMID: 39128942 Free PMC article. Review.
References
-
- Howell JY, Ramsey ML. Squamous Cell Skin Cancer. StatPearls, Treasure Island (FL), 2021.
-
- Liu‐Smith F, Jia J, Zheng Y. UV‐Induced Molecular Signaling Differences in Melanoma and Non‐melanoma Skin Cancer. Adv Exp Med Biol 2017; 996: 27–40. - PubMed
-
- Carr S, Smith C, Wernberg J. Epidemiology and Risk Factors of Melanoma. Surg Clin North Am 2020; 100: 1–12. - PubMed
-
- Flohil SC, van der Leest RJ, Dowlatshahi EA et al. Prevalence of actinic keratosis and its risk factors in the general population: the Rotterdam Study. J Invest Dermatol 2013; 133: 1971–1978. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
