

Clinical outcomes of patients with multiple courses of radiosurgery for brain metastases from non-small cell lung cancer
- PMID: 35739135
- PMCID: PMC9226031
- DOI: 10.1038/s41598-022-13853-3
Clinical outcomes of patients with multiple courses of radiosurgery for brain metastases from non-small cell lung cancer
Abstract
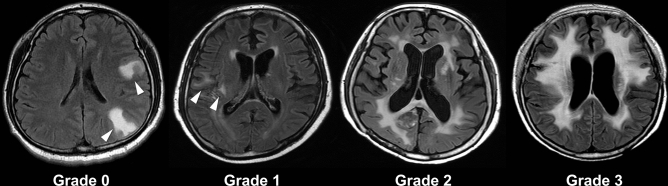
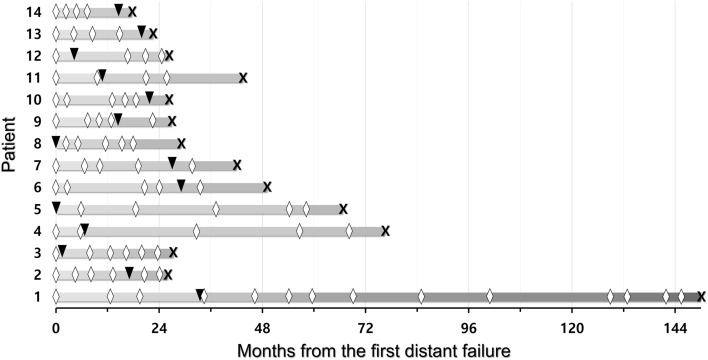
We investigated the long-term clinical outcomes of patients who underwent multiple courses (≥ 5) of gamma knife radiosurgery (GKRS) due to recurrent brain metastases (BM) from non-small cell lung cancer (NSCLC). Between December 2001 and July 2019, consecutive 2571 patients underwent GKRS for BM from NSCLC. Clinical and radiological outcomes were investigated in 76 patients who underwent GKRS ≥ 5 times. The median follow-up period after the diagnosis of NSCLC was 54.6 months (range 14.5-159.1 months). The median number of GKRS procedures per patient was six (range 5-15). Actuarial post-GKRS survival rates at 1, 2, 3, 4, and 5 years following initial GKRS were 88.1%, 79.5%, 65.3%, 51.4%, and 37.3%, respectively. No significant difference in overall survival was observed between patients (n = 22) with whole-brain radiotherapy (WBRT) and patients (n = 54) without WBRT (p = 0.076). The incidence of radiation-induced leukoencephalopathy was 64% and 18% in patients with and without WBRT, respectively (p < 0.0001). Multiple courses of SRS are a tolerable and effective treatment option for recurrent BM from NSCLC. Repeat SRS may be an alternative treatment option to avoid or delay WBRT.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Sperduto PW, et al. Secondary analysis of RTOG 9508, a phase 3 randomized trial of whole-brain radiation therapy versus WBRT plus stereotactic radiosurgery in patients with 1–3 brain metastases; Poststratified by the graded prognostic assessment (GPA) Int. J. Radiat. Oncol. Biol. Phys. 2014;90:526–531. doi: 10.1016/j.ijrobp.2014.07.002. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
