

Canine root/cortical bone relation (CRCR) and the orthodontic tooth movement
- PMID: 35739156
- PMCID: PMC9226186
- DOI: 10.1038/s41598-022-14663-3
Canine root/cortical bone relation (CRCR) and the orthodontic tooth movement
Abstract
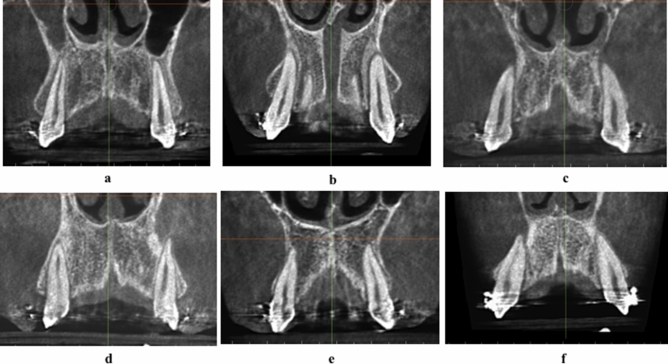
This observational study evaluates three-dimensionally the relation between the root of maxillary canine and overlying labial cortical plate of bone during orthodontic canine retraction. Eighty-four bilateral maxillary canines in 42 patients were retracted in the extraction space of first premolars, using conventional orthodontic NiTi retraction spring delivering 150gm. Three-dimensional evaluation at the cusp tip, root apex, and the overlying cortical bone was done based on Classification of Root/Cortical bone relation (CRCR) before and after canine retraction. 168 observations of the canines pre- and post-retraction showed a mean distal movement of the canine cusp tip of 3.78(± 2.05) mm, while the canine root apex was almost stationary. Scarcely, 5.4% of the canine roots and root apices persisted in the medullary bone during retraction, while 16.1% contacted the overlying cortical bone. Fenestration of the overlying cortical bone by the canine roots or root apices occurred in 78.6% of the sample. The unembellished intimacy between the canine root and apex to the overlying thick dense cortical bone might have the decelerating effect on the maxillary canine retraction. The natural bone plate labial to the maxillary canine root did not yield infront nor enlarge due to canine retraction, but else defeated the current orthodontic biomechanical implementation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures







References
-
- Krishnan V, Davidovitch Z. Cellular, molecular, and tissue-level reactions to orthodontic force. Am. J. Orthod. Dentofacial Orthop. 2006;129(469):e1–32. - PubMed
-
- Proffit, W. R. & Fields, H. W. Contemporary Orthodontics. (2000).
-
- Tweed CH. A philosophy of orthodontic treatment. Am. J. Orthod. Oral Surg. 1945;31:74–103. doi: 10.1016/S0096-6347(45)90163-3. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
