

Gene Therapy for Acquired and Genetic Cholestasis
- PMID: 35740260
- PMCID: PMC9220166
- DOI: 10.3390/biomedicines10061238
Gene Therapy for Acquired and Genetic Cholestasis
Abstract
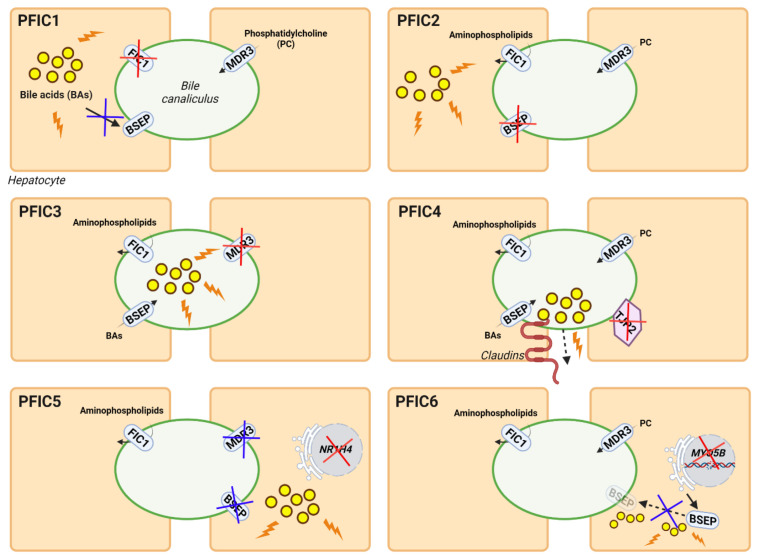
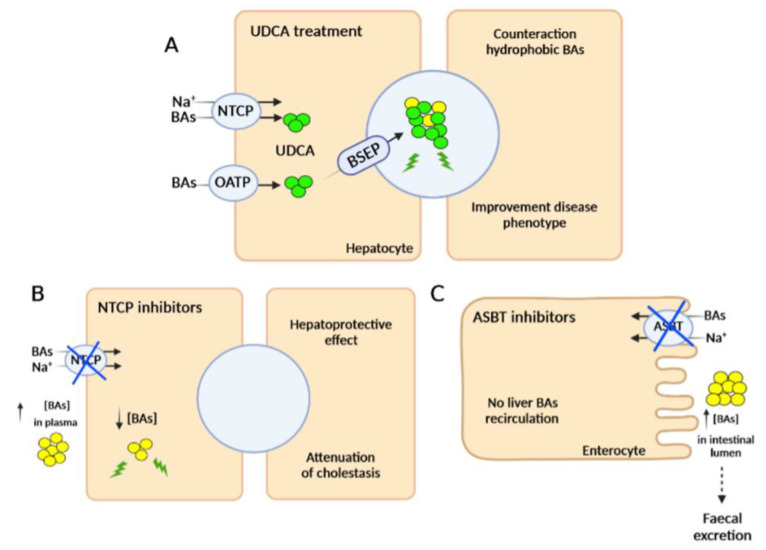
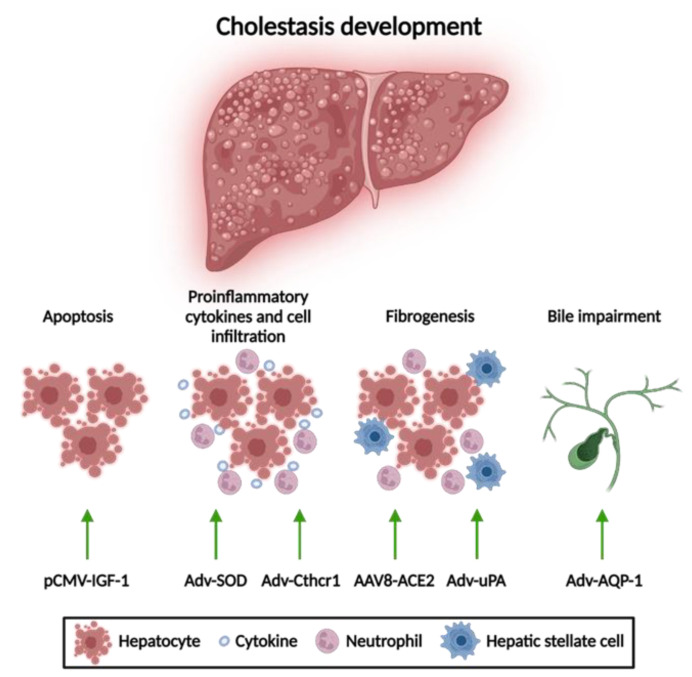
Cholestatic diseases can be caused by the dysfunction of transporters involved in hepatobiliary circulation. Although pharmacological treatments constitute the current standard of care for these diseases, none are curative, with liver transplantation being the only long-term solution for severe cholestasis, albeit with many disadvantages. Liver-directed gene therapy has shown promising results in clinical trials for genetic diseases, and it could constitute a potential new therapeutic approach for cholestatic diseases. Many preclinical gene therapy studies have shown positive results in animal models of both acquired and genetic cholestasis. The delivery of genes that reduce apoptosis or fibrosis or improve bile flow has shown therapeutic effects in rodents in which cholestasis was induced by drugs or bile duct ligation. Most studies targeting inherited cholestasis, such as progressive familial intrahepatic cholestasis (PFIC), have focused on supplementing a correct version of a mutated gene to the liver using viral or non-viral vectors in order to achieve expression of the therapeutic protein. These strategies have generated promising results in treating PFIC3 in mouse models of the disease. However, important challenges remain in translating this therapy to the clinic, as well as in developing gene therapy strategies for other types of acquired and genetic cholestasis.
Keywords: AAV; PFIC; cholestatic diseases; gene therapy.
Conflict of interest statement
N.D.W. and G.G.-A. are Vivet Therapeutics employees and hold stock in the company.
Figures
Similar articles
-
Liver-directed gene therapy results in long-term correction of progressive familial intrahepatic cholestasis type 3 in mice.J Hepatol. 2019 Jul;71(1):153-162. doi: 10.1016/j.jhep.2019.03.021. Epub 2019 Mar 29. J Hepatol. 2019. PMID: 30935993
-
Progressive familial intrahepatic cholestasis.J Clin Exp Hepatol. 2014 Mar;4(1):25-36. doi: 10.1016/j.jceh.2013.10.005. Epub 2013 Nov 23. J Clin Exp Hepatol. 2014. PMID: 25755532 Free PMC article. Review.
-
Jaundice revisited: recent advances in the diagnosis and treatment of inherited cholestatic liver diseases.J Biomed Sci. 2018 Oct 26;25(1):75. doi: 10.1186/s12929-018-0475-8. J Biomed Sci. 2018. PMID: 30367658 Free PMC article. Review.
-
Prevention of Cholestatic Liver Disease and Reduced Tumorigenicity in a Murine Model of PFIC Type 3 Using Hybrid AAV-piggyBac Gene Therapy.Hepatology. 2019 Dec;70(6):2047-2061. doi: 10.1002/hep.30773. Epub 2019 Jun 26. Hepatology. 2019. PMID: 31099022
-
Genetic cholestasis, causes and consequences for hepatobiliary transport.Liver Int. 2003 Oct;23(5):315-22. doi: 10.1034/j.1478-3231.2003.00856.x. Liver Int. 2003. PMID: 14708891 Review.
Cited by
-
Clinical and genetic characterization of pediatric patients with progressive familial intrahepatic cholestasis type 3 (PFIC3): identification of 14 novel ABCB4 variants and review of the literatures.Orphanet J Rare Dis. 2022 Dec 22;17(1):445. doi: 10.1186/s13023-022-02597-y. Orphanet J Rare Dis. 2022. PMID: 36550572 Free PMC article. Review.
-
Hepatic Nuclear Receptors in Cholestasis-to-Cholangiocarcinoma Pathology.Am J Pathol. 2025 Mar;195(3):409-421. doi: 10.1016/j.ajpath.2024.07.023. Epub 2024 Sep 24. Am J Pathol. 2025. PMID: 39326734 Free PMC article. Review.
-
Progressive Familial Intrahepatic Cholestasis Type 2 in an Infant: Diagnostic Challenges and Multidisciplinary Management.Cureus. 2024 Dec 25;16(12):e76355. doi: 10.7759/cureus.76355. eCollection 2024 Dec. Cureus. 2024. PMID: 39867052 Free PMC article.
-
Genotypes and different clinical variants between children and adults in progressive familial intrahepatic cholestasis: a state-of-the-art review.Orphanet J Rare Dis. 2025 Feb 21;20(1):80. doi: 10.1186/s13023-025-03599-2. Orphanet J Rare Dis. 2025. PMID: 39984942 Free PMC article. Review.
-
Advances in Pathogenesis and Therapeutics of Hepatobiliary Diseases.Biomedicines. 2023 Apr 10;11(4):1140. doi: 10.3390/biomedicines11041140. Biomedicines. 2023. PMID: 37189758 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
