

Ability of Delta Radiomics to Predict a Complete Pathological Response in Patients with Loco-Regional Rectal Cancer Addressed to Neoadjuvant Chemo-Radiation and Surgery
- PMID: 35740669
- PMCID: PMC9221458
- DOI: 10.3390/cancers14123004
Ability of Delta Radiomics to Predict a Complete Pathological Response in Patients with Loco-Regional Rectal Cancer Addressed to Neoadjuvant Chemo-Radiation and Surgery
Abstract
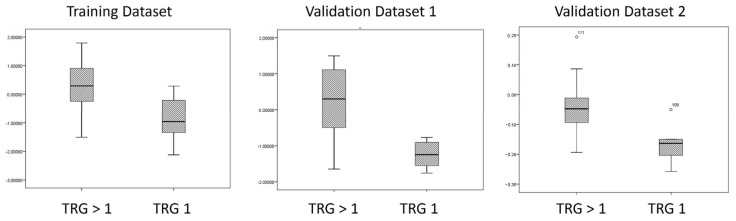
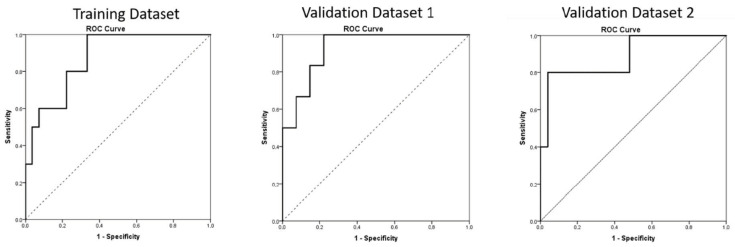
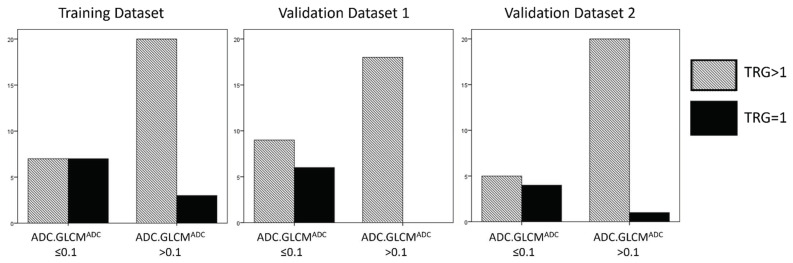
We performed a pilot study to evaluate the use of MRI delta texture analysis (D-TA) as a methodological item able to predict the frequency of complete pathological responses and, consequently, the outcome of patients with locally advanced rectal cancer addressed to neoadjuvant chemoradiotherapy (C-RT) and subsequently, to radical surgery. In particular, we carried out a retrospective analysis including 100 patients with locally advanced rectal adenocarcinoma who received C-RT and then radical surgery in three different oncological institutions between January 2013 and December 2019. Our experimental design was focused on the evaluation of the gross tumor volume (GTV) at baseline and after C-RT by means of MRI, which was contoured on T2, DWI, and ADC sequences. Multiple texture parameters were extracted by using a LifeX Software, while D-TA was calculated as percentage of variations in the two time points. Both univariate and multivariate analysis (logistic regression) were, therefore, carried out in order to correlate the above-mentioned TA parameters with the frequency of pathological responses in the examined patients' population focusing on the detection of complete pathological response (pCR, with no viable cancer cells: TRG 1) as main statistical endpoint. ROC curves were performed on three different datasets considering that on the 21 patients, only 21% achieved an actual pCR. In our training dataset series, pCR frequency significantly correlated with ADC GLCM-Entropy only, when univariate and binary logistic analysis were performed (AUC for pCR was 0.87). A confirmative binary logistic regression analysis was then repeated in the two remaining validation datasets (AUC for pCR was 0.92 and 0.88, respectively). Overall, these results support the hypothesis that D-TA may have a significant predictive value in detecting the occurrence of pCR in our patient series. If confirmed in prospective and multicenter trials, these results may have a critical role in the selection of patients with locally advanced rectal cancer who may benefit form radical surgery after neoadjuvant chemoradiotherapy.
Keywords: MRI; neoadjuvant chemo-radiation; rectal cancer; texture analysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
[A prediction model of pathological complete response in patients with locally advanced rectal cancer after PD-1 antibody combined with total neoadjuvant chemoradiotherapy based on MRI radiomics].Zhonghua Wei Chang Wai Ke Za Zhi. 2022 Mar 25;25(3):228-234. doi: 10.3760/cma.j.cn441530-20211222-00527. Zhonghua Wei Chang Wai Ke Za Zhi. 2022. PMID: 35340172 Clinical Trial. Chinese.
-
[Application value of texture analysis of magnetic resonance images in prediction of neoadjuvant chemoradiotherapy efficacy for rectal cancer].Zhonghua Wei Chang Wai Ke Za Zhi. 2018 Sep 25;21(9):1051-1058. Zhonghua Wei Chang Wai Ke Za Zhi. 2018. PMID: 30269327 Chinese.
-
MRI-based delta-radiomics are predictive of pathological complete response after neoadjuvant chemoradiotherapy in locally advanced rectal cancer.Acad Radiol. 2021 Nov;28 Suppl 1:S95-S104. doi: 10.1016/j.acra.2020.10.026. Epub 2020 Nov 12. Acad Radiol. 2021. PMID: 33189550
-
MRI T2-weighted sequences-based texture analysis (TA) as a predictor of response to neoadjuvant chemo-radiotherapy (nCRT) in patients with locally advanced rectal cancer (LARC).Radiol Med. 2020 Dec;125(12):1216-1224. doi: 10.1007/s11547-020-01215-w. Epub 2020 May 14. Radiol Med. 2020. PMID: 32410063
-
Radiomics analysis of multiparametric MRI for prediction of pathological complete response to neoadjuvant chemoradiotherapy in locally advanced rectal cancer.Eur Radiol. 2019 Mar;29(3):1211-1220. doi: 10.1007/s00330-018-5683-9. Epub 2018 Aug 20. Eur Radiol. 2019. PMID: 30128616
Cited by
-
Capecitabine-A "Permanent Mission" in Head and Neck Cancers "War Council"?J Clin Med. 2022 Sep 23;11(19):5582. doi: 10.3390/jcm11195582. J Clin Med. 2022. PMID: 36233450 Free PMC article. Review.
-
MRI-based radiomics for predicting pathological complete response after neoadjuvant chemoradiotherapy in locally advanced rectal cancer: a systematic review and meta-analysis.Front Oncol. 2025 Mar 10;15:1550838. doi: 10.3389/fonc.2025.1550838. eCollection 2025. Front Oncol. 2025. PMID: 40129922 Free PMC article.
-
Machine learning in predicting pathological complete response to neoadjuvant chemoradiotherapy in rectal cancer using MRI: a systematic review and meta-analysis.Br J Radiol. 2024 Jun 18;97(1159):1243-1254. doi: 10.1093/bjr/tqae098. Br J Radiol. 2024. PMID: 38730550 Free PMC article.
-
Predictive Potential of Contrast-Enhanced MRI-Based Delta-Radiomics for Chemoradiation Responsiveness in Muscle-Invasive Bladder Cancer.Diagnostics (Basel). 2025 Mar 21;15(7):801. doi: 10.3390/diagnostics15070801. Diagnostics (Basel). 2025. PMID: 40218151 Free PMC article.
-
MRI-based radiomics to predict neoadjuvant chemoradiotherapy outcomes in locally advanced rectal cancer: A multicenter study.Clin Transl Radiat Oncol. 2022 Nov 17;38:175-182. doi: 10.1016/j.ctro.2022.11.009. eCollection 2023 Jan. Clin Transl Radiat Oncol. 2022. PMID: 36471751 Free PMC article.
References
-
- van Gijn W., Marijnen C.A., Nagtegaal I.D., Kranenbarg E.M., Putter H., Wiggers T., Rutten H.J., Pahlman L., Glimelius B., van de Velde C.J., et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial. Lancet Oncol. 2011;12:575–582. doi: 10.1016/S1470-2045(11)70097-3. - DOI - PubMed
-
- Sauer R., Liersch T., Merkel S., Fietkau R., Hohenberger W., Hess C., Becker H., Raab H.R., Villanueva M.T., Witzigmann H., et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: Results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J. Clin. Oncol. 2012;30:1926–1933. doi: 10.1200/JCO.2011.40.1836. - DOI - PubMed
-
- Sebag-Montefiore D., Stephens R.J., Steele R., Monson J., Grieve R., Khanna S., Quirke P., Couture J., de Metz C., Myint A.S., et al. Preoperative radiotherapy versus selective postoperative chemoradiotherapy in patients with rectal cancer (MRC CR07 and NCIC-CTG C016): A multicentre, randomised trial. Lancet. 2009;373:811–820. doi: 10.1016/S0140-6736(09)60484-0. - DOI - PMC - PubMed
-
- Granata V., Faggioni L., Grassi R., Fusco R., Reginelli A., Rega D., Maggialetti N., Buccicardi D., Frittoli B., Rengo M., et al. Structured reporting of computed tomography in the staging of colon cancer: A Delphi consensus proposal. Radiol. Med. 2022;127:21–29. doi: 10.1007/s11547-021-01418-9. - DOI - PMC - PubMed
-
- Link K.H., Kornmann M., Staib L., Kreuser E.D., Gaus W., Röttinger E., Suhr P., Maulbecker-Armstrong C., Danenberg P., Danenberg K., et al. Patient-centered developments in colon- and rectal cancer with a multidisciplinary international team: From translational research to national guidelines. World J. Gastrointest. Surg. 2021;13:1597–1614. doi: 10.4240/wjgs.v13.i12.1597. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
