

Conformity between Pacifier Design and Palate Shape in Preterm and Term Infants Considering Age-Specific Palate Size, Facial Profile and Lip Thickness
- PMID: 35740710
- PMCID: PMC9221625
- DOI: 10.3390/children9060773
Conformity between Pacifier Design and Palate Shape in Preterm and Term Infants Considering Age-Specific Palate Size, Facial Profile and Lip Thickness
Abstract
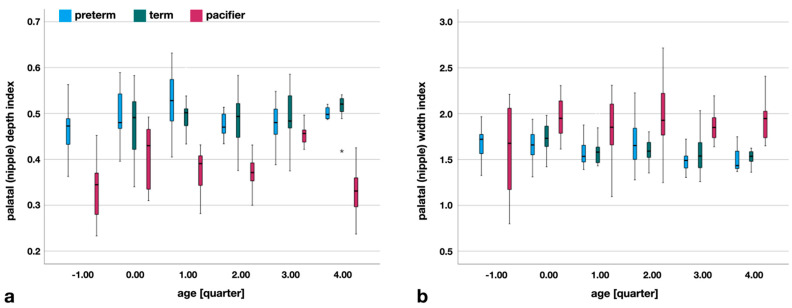
This retrospective case-control study is the first to examine the spatial conformity between pacifiers and palates in 39 preterm infants (12 females, 27 males) and 34 term infants (19 females, 15 males), taking into account the facial-soft-tissue profile and thickness. The shape of 74 available pacifiers was spatially matched to the palate, and conformity was examined using width, height, and length measurements. In summary, the size concept of pacifiers is highly variable and does not follow a growth pattern, like infant palates do. Pacifiers are too undersized in width, length, and height to physiologically fit the palate structures from 0 to 14 months of age. There are two exceptions, but only for premature palates: the palatal depth index at 9−11 months of age, which has no clinical meaning, and the nipple length at <37 weeks of age, which bears a resemblance to the maternal nipple during non-nutritive sucking. It can be concluded that the age-size concept of the studied pacifiers does not correspond to any natural growth pattern. Physiologically aligned, pacifiers do not achieve the age-specific dimensions of the palate. The effects attributed to the products on oral health in term infants cannot be supposed.
Keywords: growth; non-nutritive sucking; pacifier; palates; preterm infants; term infants.
Conflict of interest statement
The authors declare no conflict of interest.
Figures








Similar articles
-
Functional comparison of pacifiers using finite element analysis.BMC Oral Health. 2022 Mar 2;22(1):49. doi: 10.1186/s12903-022-02087-4. BMC Oral Health. 2022. PMID: 35236336 Free PMC article.
-
Effects of pacifier use on transition to full breastfeeding and sucking skills in preterm infants: a randomised controlled trial.J Clin Nurs. 2017 Jul;26(13-14):2055-2063. doi: 10.1111/jocn.13617. Epub 2017 Mar 21. J Clin Nurs. 2017. PMID: 27754572 Clinical Trial.
-
Effects of Pacifier Use on Transition Time from Gavage to Breastfeeding in Preterm Infants: A Randomized Controlled Trial.Breastfeed Med. 2018 Jul/Aug;13(6):433-437. doi: 10.1089/bfm.2018.0031. Epub 2018 Jun 18. Breastfeed Med. 2018. PMID: 29912580 Clinical Trial.
-
How might non nutritional sucking protect from sudden infant death syndrome.Med Hypotheses. 2020 Oct;143:109868. doi: 10.1016/j.mehy.2020.109868. Epub 2020 May 22. Med Hypotheses. 2020. PMID: 32480251 Review.
-
Palatal development of preterm and low birthweight infants compared to term infants - What do we know? Part 2: The palate of the preterm/low birthweight infant.Head Face Med. 2005 Oct 28;1:9. doi: 10.1186/1746-160X-1-9. Head Face Med. 2005. PMID: 16270909 Free PMC article. Review.
Cited by
-
Influence of pacifier design on pacifier-palate contact: a finite element analysis.Head Face Med. 2025 Jul 11;21(1):50. doi: 10.1186/s13005-025-00525-6. Head Face Med. 2025. PMID: 40640845 Free PMC article.
References
-
- Del Conte Zardetto C.G., Rodrigues C.R.M.D., Stefani F.M. Effects of different pacifiers on the primary dentition and oral myofunctional structures of preschool children. Pediatr. Dent. 2002;24:552–560. - PubMed
LinkOut - more resources
Full Text Sources
