

The Underlying Role of the Glymphatic System and Meningeal Lymphatic Vessels in Cerebral Small Vessel Disease
- PMID: 35740873
- PMCID: PMC9221030
- DOI: 10.3390/biom12060748
The Underlying Role of the Glymphatic System and Meningeal Lymphatic Vessels in Cerebral Small Vessel Disease
Erratum in
-
Correction: Tian et al. The Underlying Role of the Glymphatic System and Meningeal Lymphatic Vessels in Cerebral Small Vessel Disease. Biomolecules 2022, 12, 748.Biomolecules. 2023 Apr 21;13(4):705. doi: 10.3390/biom13040705. Biomolecules. 2023. PMID: 37189464 Free PMC article.
Abstract
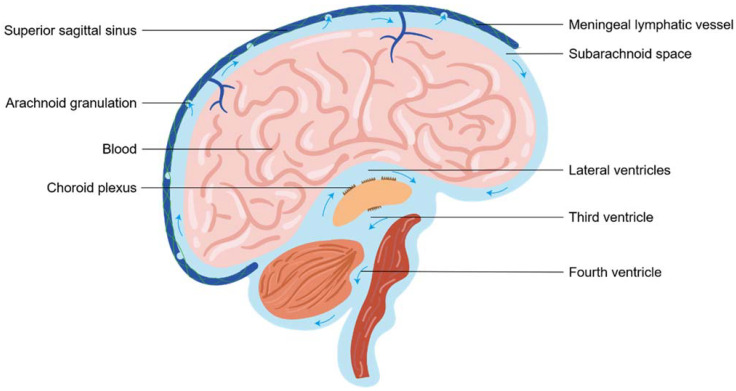
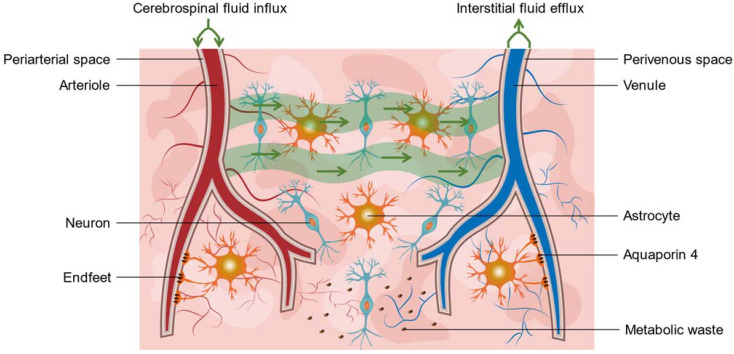
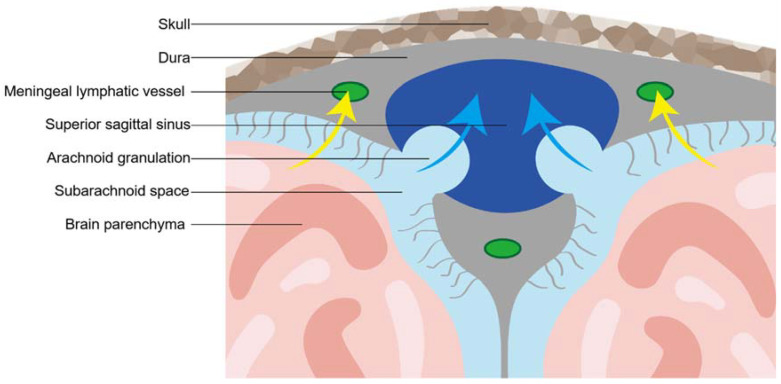
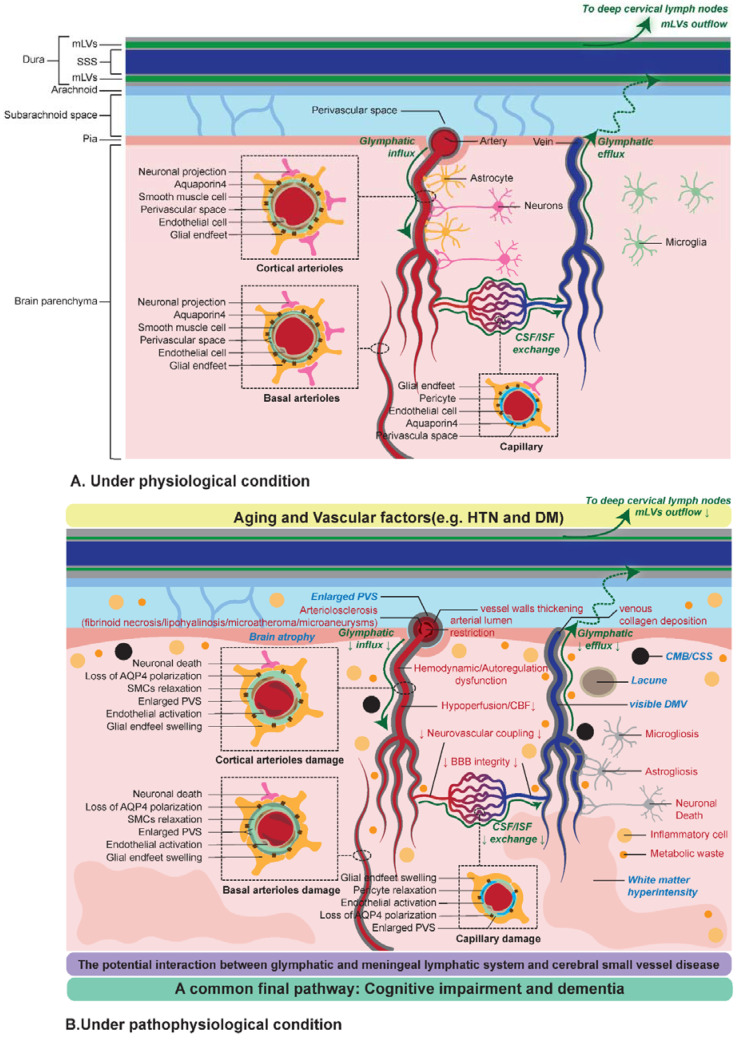
There is a growing prevalence of vascular cognitive impairment (VCI) worldwide, and most research has suggested that cerebral small vessel disease (CSVD) is the main contributor to VCI. Several potential physiopathologic mechanisms have been proven to be involved in the process of CSVD, such as blood-brain barrier damage, small vessels stiffening, venous collagenosis, cerebral blood flow reduction, white matter rarefaction, chronic ischaemia, neuroinflammation, myelin damage, and subsequent neurodegeneration. However, there still is a limited overall understanding of the sequence and the relative importance of these mechanisms. The glymphatic system (GS) and meningeal lymphatic vessels (mLVs) are the analogs of the lymphatic system in the central nervous system (CNS). As such, these systems play critical roles in regulating cerebrospinal fluid (CSF) and interstitial fluid (ISF) transport, waste clearance, and, potentially, neuroinflammation. Accumulating evidence has suggested that the glymphatic and meningeal lymphatic vessels played vital roles in animal models of CSVD and patients with CSVD. Given the complexity of CSVD, it was significant to understand the underlying interaction between glymphatic and meningeal lymphatic transport with CSVD. Here, we provide a novel framework based on new advances in main four aspects, including vascular risk factors, potential mechanisms, clinical subtypes, and cognition, which aims to explain how the glymphatic system and meningeal lymphatic vessels contribute to the progression of CSVD and proposes a comprehensive insight into the novel therapeutic strategy of CSVD.
Keywords: cerebral small vessel disease; cerebrospinal fluid; glymphatic system; meningeal lymphatic vessel.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gorelick P.B., Scuteri A., Black S.E., Decarli C., Greenberg S.M., Iadecola C., Launer L.J., Laurent S., Lopez O.L., Nyenhuis D., et al. Vascular contributions to cognitive impairment and dementia: A statement for healthcare professionals from the american heart association/american stroke association. Stroke. 2011;42:2672–2713. doi: 10.1161/STR.0b013e3182299496. - DOI - PMC - PubMed
-
- De Leeuw F.E., de Groot J.C., Achten E., Oudkerk M., Ramos L.M., Heijboer R., Hofman A., Jolles J., van Gijn J., Breteler M.M. Prevalence of cerebral white matter lesions in elderly people: A population based magnetic resonance imaging study. The Rotterdam Scan Study. J. Neurol. Neurosurg. Psychiatry. 2001;70:9–14. doi: 10.1136/jnnp.70.1.9. - DOI - PMC - PubMed
-
- Wardlaw J.M., Smith E.E., Biessels G.J., Cordonnier C., Fazekas F., Frayne R., Lindley R.I., O’Brien J.T., Barkhof F., Benavente O.R., et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013;12:822–838. doi: 10.1016/S1474-4422(13)70124-8. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
