

Current and Novel Therapeutic Approaches for Treatment of Diabetic Macular Edema
- PMID: 35741079
- PMCID: PMC9221813
- DOI: 10.3390/cells11121950
Current and Novel Therapeutic Approaches for Treatment of Diabetic Macular Edema
Abstract
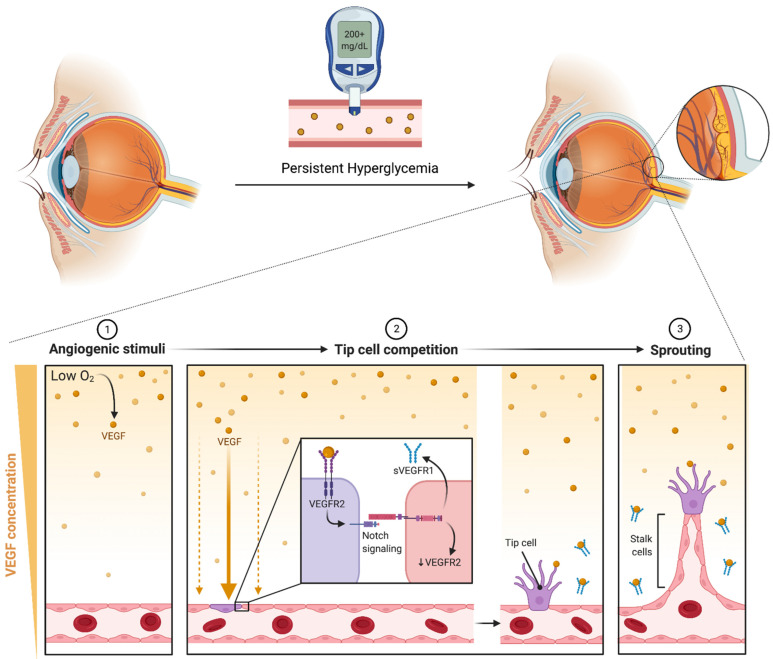
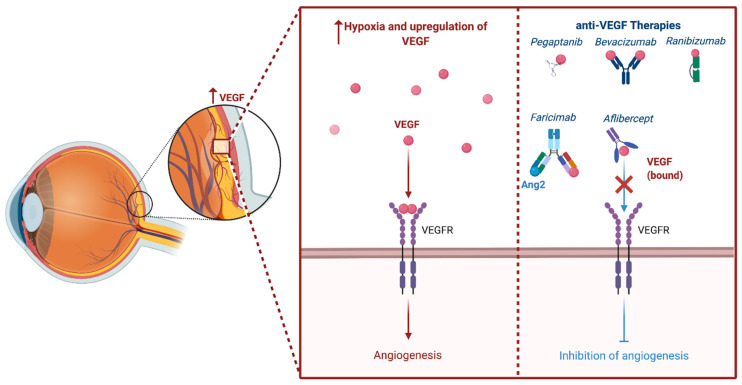
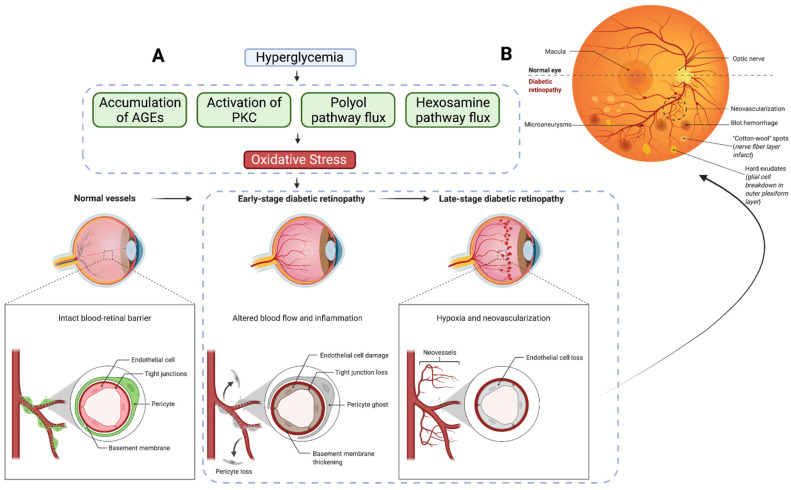
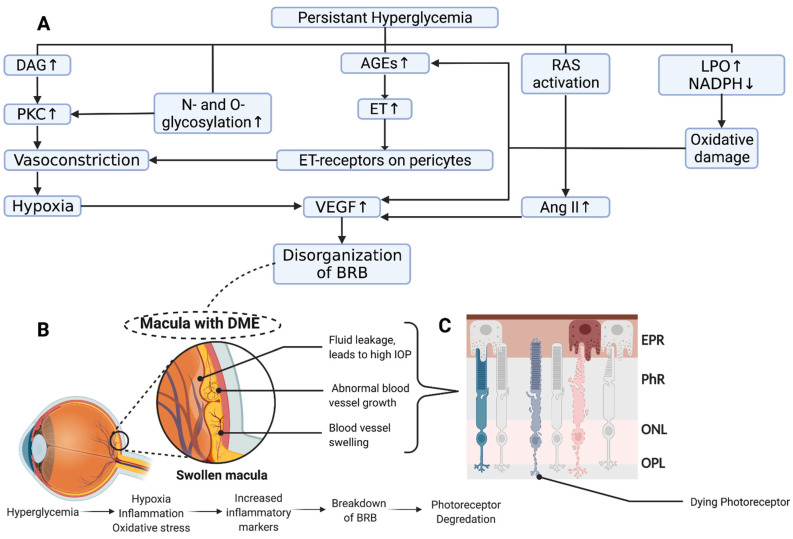
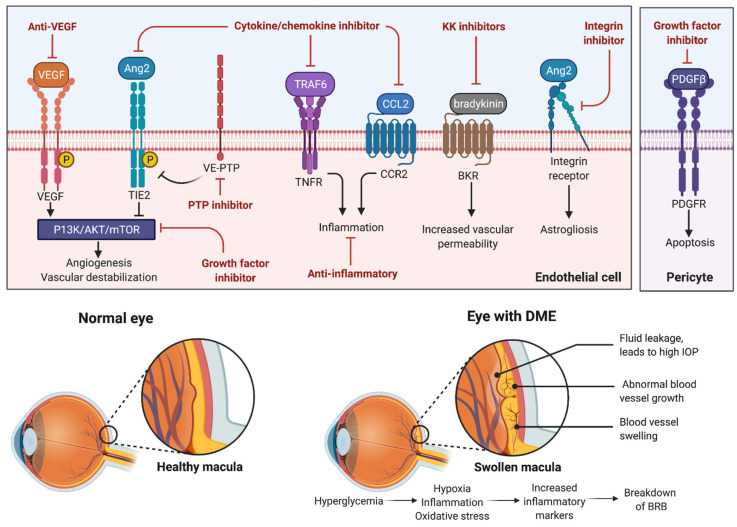
Diabetic macular edema (DME) is a major ocular complication of diabetes mellitus (DM), leading to significant visual impairment. DME's pathogenesis is multifactorial. Focal edema tends to occur when primary metabolic abnormalities lead to a persistent hyperglycemic state, causing the development of microaneurysms, often with extravascular lipoprotein in a circinate pattern around the focal leakage. On the other hand, diffusion edema is due to a generalized breakdown of the inner blood-retinal barrier, leading to profuse early leakage from the entire capillary bed of the posterior pole with the subsequent extravasation of fluid into the extracellular space. The pathogenesis of DME occurs through the interaction of multiple molecular mediators, including the overexpression of several growth factors, including vascular endothelial growth factor (VEGF), insulin-like growth factor-1, angiopoietin-1, and -2, stromal-derived factor-1, fibroblast growth factor-2, and tumor necrosis factor. Synergistically, these growth factors mediate angiogenesis, protease production, endothelial cell proliferation, and migration. Treatment for DME generally involves primary management of DM, laser photocoagulation, and pharmacotherapeutics targeting mediators, namely, the anti-VEGF pathway. The emergence of anti-VEGF therapies has resulted in significant clinical improvements compared to laser therapy alone. However, multiple factors influencing the visual outcome after anti-VEGF treatment and the presence of anti-VEGF non-responders have necessitated the development of new pharmacotherapies. In this review, we explore the pathophysiology of DME and current management strategies. In addition, we provide a comprehensive analysis of emerging therapeutic approaches to the treatment of DME.
Keywords: VEGF; diabetic macular edema; intravitreal injection; laser photocoagulation; novel pharmacotherapy; therapeutics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kumar V., Abbas A.K., Aster J.C., Perkins J.A. Robbins Basic Pathology. 10th ed. Elsevier; Philadelphia, PA, USA: 2018. p. xiv.935p
-
- GBD 2019 Blindness and Vision Impairment Collaborators on behalf of the Vision Loss Expert Group of the Global Burden of Disease Study Causes of blindness and vision impairment in 2020 and trends over 30 years, and prevalence of avoidable blindness in relation to VISION 2020: The Right to Sight: An analysis for the Global Burden of Disease Study. Lancet Glob. Health. 2021;9:e144–e160. doi: 10.1016/S2214-109X(20)30489-7. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
