

Translation of a Protease Turnover Assay for Clinical Discrimination of Mucinous Pancreatic Cysts
- PMID: 35741154
- PMCID: PMC9222202
- DOI: 10.3390/diagnostics12061343
Translation of a Protease Turnover Assay for Clinical Discrimination of Mucinous Pancreatic Cysts
Abstract
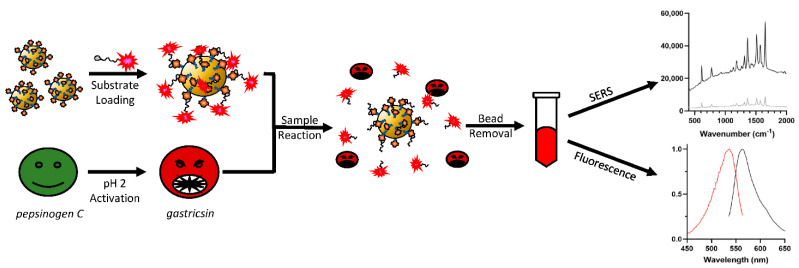
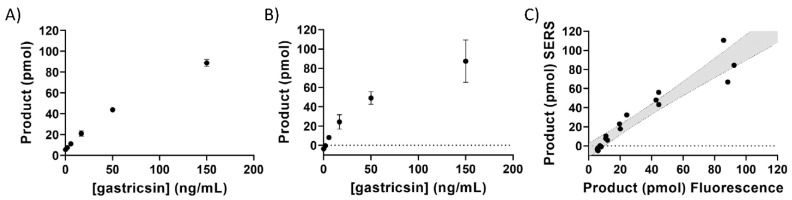
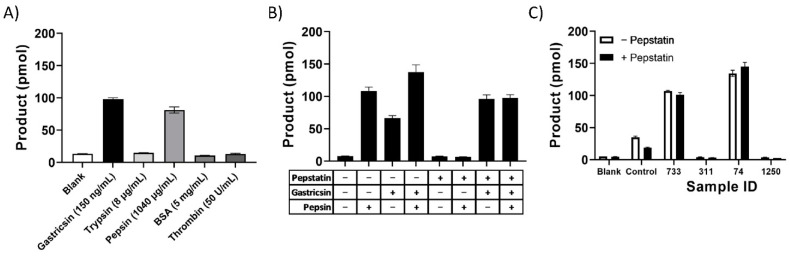
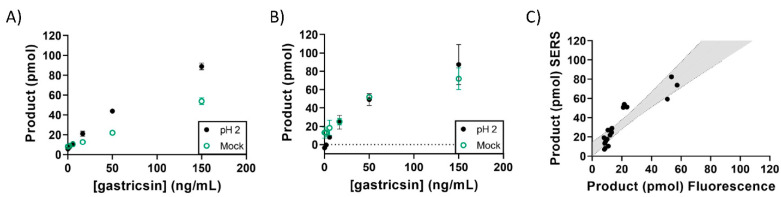
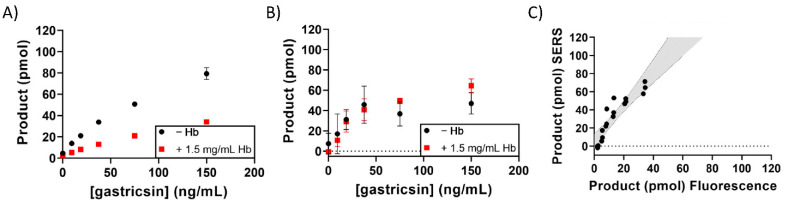
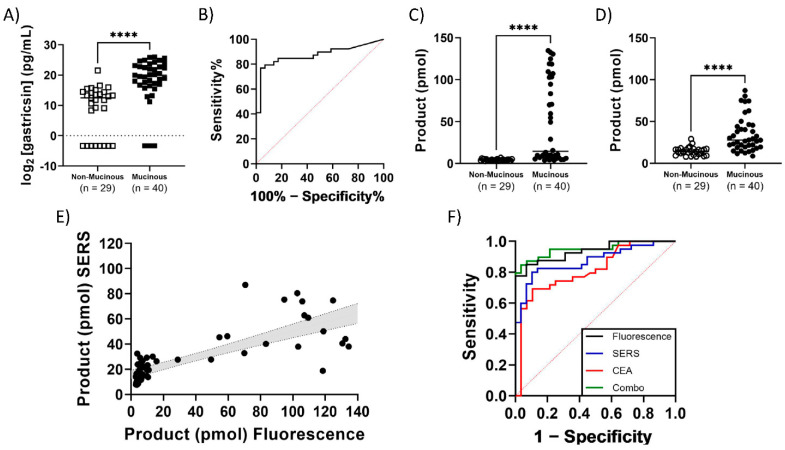
The classification of pancreatic cyst fluids can provide a basis for the early detection of pancreatic cancer while eliminating unnecessary procedures. A candidate biomarker, gastricsin (pepsin C), was found to be present in potentially malignant mucinous pancreatic cyst fluids. A gastricsin activity assay using a magnetic bead-based platform has been developed using immobilized peptide substrates selective for gastricsin bearing a dimeric rhodamine dye. The unique dye structure allows quantitation of enzyme-cleaved product by both fluorescence and surface enhanced Raman spectroscopy (SERS). The performance of this assay was compared with ELISA assays of pepsinogen C and the standard of care, carcinoembryonic antigen (CEA), in the same clinical sample cohort. A retrospective cohort of mucinous (n = 40) and non-mucinous (n = 29) classes of pancreatic cyst fluid samples were analyzed using the new protease activity assay. For both assay detection modes, successful differentiation of mucinous and non-mucinous cyst fluid was achieved using 1 µL clinical samples. The activity-based assays in combination with CEA exhibit optimal sensitivity and specificity of 87% and 93%, respectively. The use of this gastricsin activity assay requires a minimal volume of clinical specimen, offers a rapid assay time, and shows improvements in the differentiation of mucinous and non-mucinous cysts using an accurate standardized readout of product formation, all without interfering with the clinical standard of care.
Keywords: early detection; matrix effects; minimal volume; mucinous; non-mucinous; pancreatic cancer; surface-enhanced Raman spectroscopy (SERS).
Conflict of interest statement
K.B., U.C.R. and D.A.S. were funded by Amplified Sciences, and disclose financial incentives with Amplified Sciences via stock options. V.J.D. is CSO of Amplified Sciences, and has financial connections therein. C.S.C. also has stock option considerations from Amplified Sciences, as well as Alaunus Biosciences. F.C. has stock options from Alaunus Biosciences.
Figures
References
-
- Cancer Facts & Figures 2022 American Cancer Society. [(accessed on 2 February 2022)]. Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts....
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
