

Predictors for COVID-19 Complete Remission with HRCT Pattern Evolution: A Monocentric, Prospective Study
- PMID: 35741206
- PMCID: PMC9221666
- DOI: 10.3390/diagnostics12061397
Predictors for COVID-19 Complete Remission with HRCT Pattern Evolution: A Monocentric, Prospective Study
Abstract
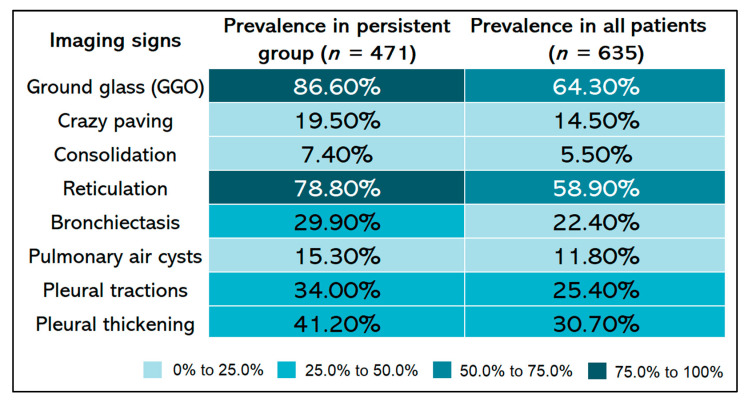
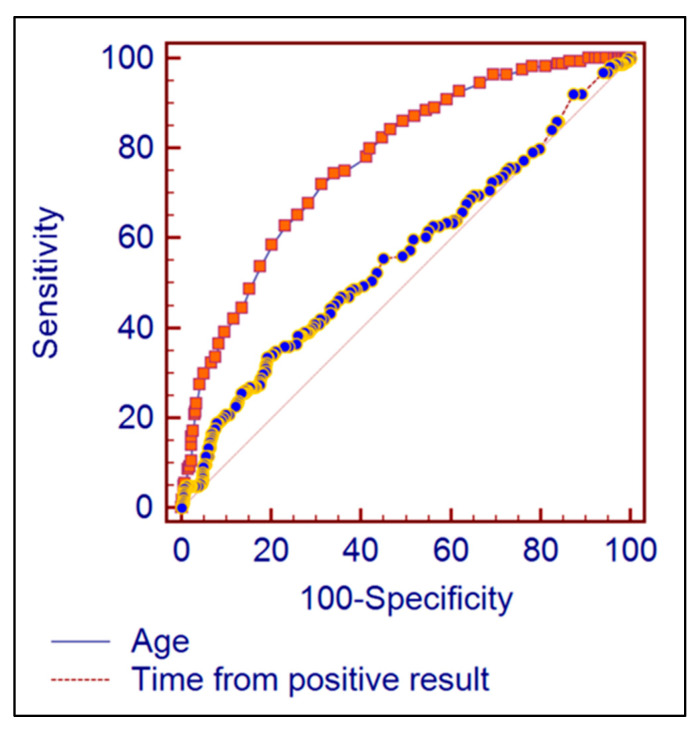
There are growing concerns that some COVID-19 survivors may acquire fibrosis and other irreversible lung abnormalities. The purpose of this prospective study was to assess the rate and predictors of complete resolution of COVID-19 pneumonia by pursuing a hypothetical relation between time and imaging pattern evolution using HRCT findings. A monocentric prospective cohort study with a consecutive-case enrolment design was implemented during a five-month period, having a total of 683 post-COVID patients eligible for inclusion and 635 evaluations with complete follow-up for chest HRCT. The target for post-COVID evaluations consisted of performing HRCT 90 days after a confirmed SARS-CoV-2 infection. The studied patients had an average age of 54 years, ranging between 18 and 85 years old, and an average duration from the first symptoms until HRCT was performed of 74 days. At the post-COVID follow-up, 25.8% had a complete imagistic remission. The most common appearance with HRCT was “ground glass” in 86.6% in patients with persistent COVID-19, followed by reticulations, present in 78.8%, and respectively pleural thickening in 41.2% of cases. The mean total HRCT scores were statistically significantly higher in patients older than 65 years (10.6 ± 6.0) compared to the 40−65 group (6.1 ± 6.1) and the 18−40 age group (2.7 ± 4.8) (p < 0.001). Chest HRCT is a “time window” in documenting temporal persistent radiologic features of lung injury 90 days after SARS-CoV-2 infection, determining the pathologic basis of so-called “long COVID”. The complete remission was associated with a significantly higher average follow-up period and a significantly lower average patient age. Persistent HRCT features of ground glass, reticulation, and pleural thickening are associated with a higher total CT score and older age.
Keywords: COVID-19; HRCT; SARS-CoV-2 infection; disease remission; imaging studies; prediction model.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Mohanty S.K., Satapathy A., Naidu M.M., Mukhopadhyay S., Sharma S., Barton L.M., Stroberg E., Duval E.J., Pradhan D., Tzankovet A., et al. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19)—anatomic pathology perspective on current knowledge. Diagn. Pathol. 2020;15:103. doi: 10.1186/s13000-020-01017-8. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
