

Deep-Learning-Based Thrombus Localization and Segmentation in Patients with Posterior Circulation Stroke
- PMID: 35741209
- PMCID: PMC9222185
- DOI: 10.3390/diagnostics12061400
Deep-Learning-Based Thrombus Localization and Segmentation in Patients with Posterior Circulation Stroke
Abstract
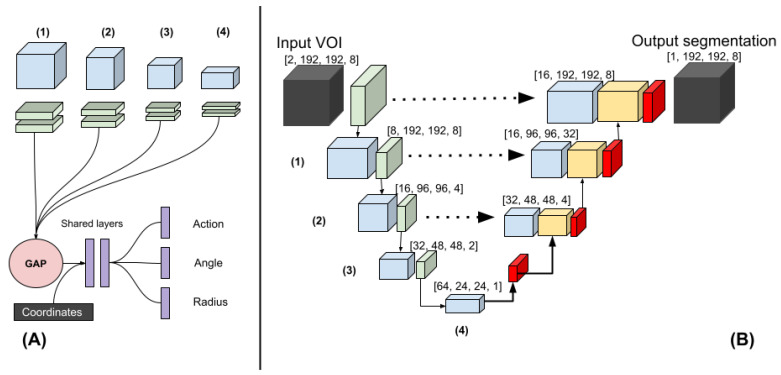
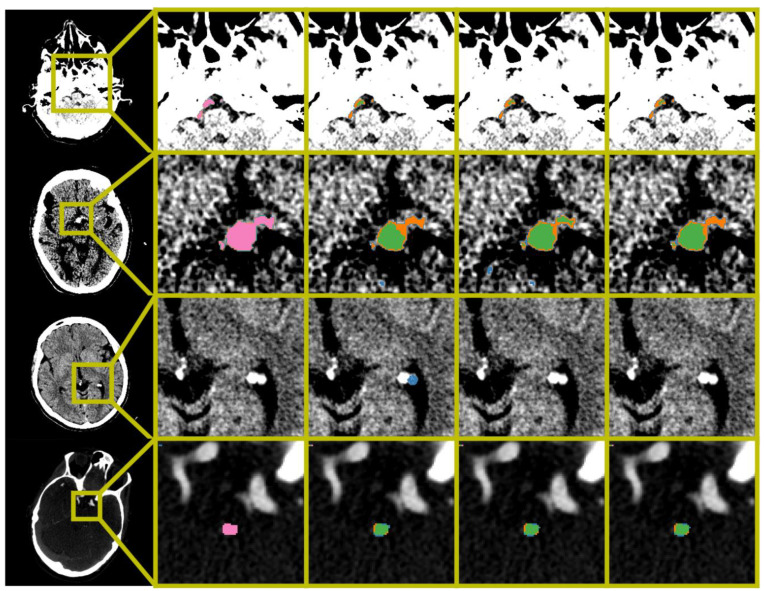
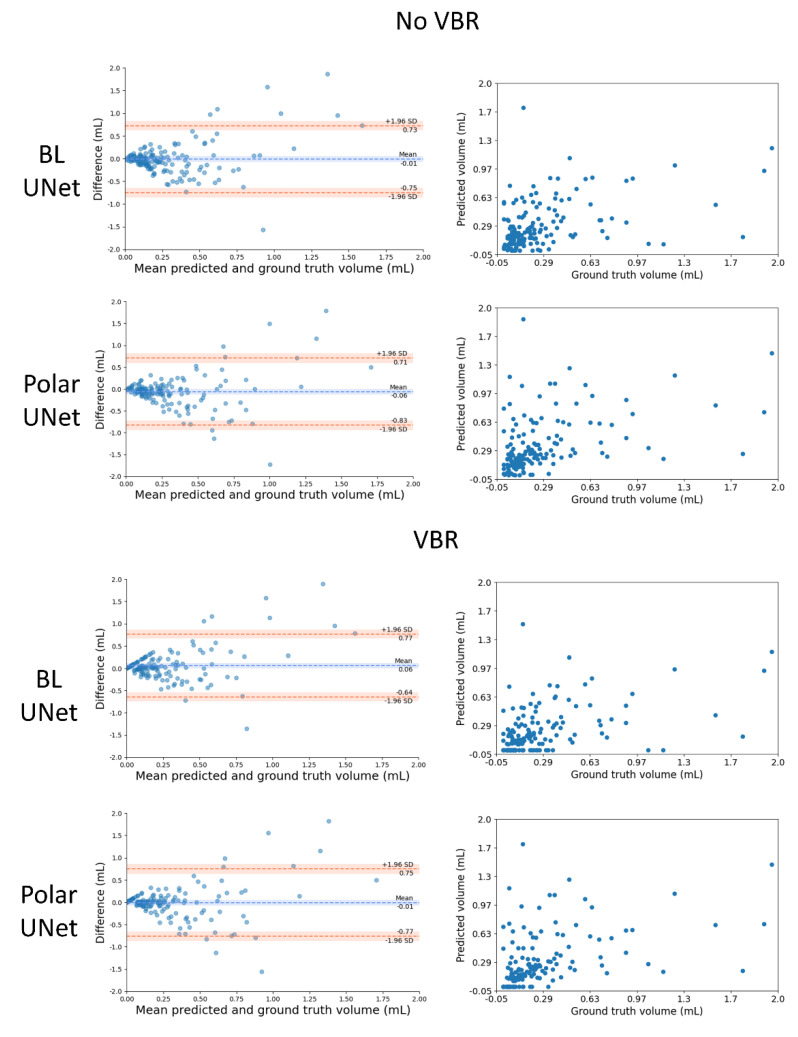
Thrombus volume in posterior circulation stroke (PCS) has been associated with outcome, through recanalization. Manual thrombus segmentation is impractical for large scale analysis of image characteristics. Hence, in this study we develop the first automatic method for thrombus localization and segmentation on CT in patients with PCS. In this multi-center retrospective study, 187 patients with PCS from the MR CLEAN Registry were included. We developed a convolutional neural network (CNN) that segments thrombi and restricts the volume-of-interest (VOI) to the brainstem (Polar-UNet). Furthermore, we reduced false positive localization by removing small-volume objects, referred to as volume-based removal (VBR). Polar-UNet is benchmarked against a CNN that does not restrict the VOI (BL-UNet). Performance metrics included the intra-class correlation coefficient (ICC) between automated and manually segmented thrombus volumes, the thrombus localization precision and recall, and the Dice coefficient. The majority of the thrombi were localized. Without VBR, Polar-UNet achieved a thrombus localization recall of 0.82, versus 0.78 achieved by BL-UNet. This high recall was accompanied by a low precision of 0.14 and 0.09. VBR improved precision to 0.65 and 0.56 for Polar-UNet and BL-UNet, respectively, with a small reduction in recall to 0.75 and 0.69. The Dice coefficient achieved by Polar-UNet was 0.44, versus 0.38 achieved by BL-UNet with VBR. Both methods achieved ICCs of 0.41 (95% CI: 0.27-0.54). Restricting the VOI to the brainstem improved the thrombus localization precision, recall, and segmentation overlap compared to the benchmark. VBR improved thrombus localization precision but lowered recall.
Keywords: CTA; NCCT; deep learning; localization; posterior stroke; segmentation; thrombus.
Conflict of interest statement
H.A. Marquering is a cofounder and shareholder of Nico.Lab. I. Išgum is a cofounder, scientific lead, and shareholder of Quantib-U. C.B.L.M. Majoie is a shareholder of Nico.Lab and has received speakers’ bureau fees from Stryker (paid to institution). D.W.J. Dippel received honoraria from Stryker (paid to institution). W.H. van Zwam received speaker fees from Stryker, NicoLab, and Cernovus, and consultation fees from Philips (all paid to institution). S.A.P. Cornelissen has no competing interests.
Figures
References
-
- Pirson F.A.V., Boodt N., Brouwer J., Bruggeman A.A.E., den Hartog S.J., Goldhoorn R.-J.B., Langezaal L.C.M., Staals J., van Zwam W.H., van der Leij C., et al. Endovascular Treatment for Posterior Circulation Stroke in Routine Clinical Practice: Results of the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands Registry. Stroke. 2021:STROKEAHA121034786. doi: 10.1161/STROKEAHA.121.034786. - DOI - PubMed
LinkOut - more resources
Full Text Sources
