

Secondary (Late) Developmental Dysplasia of the Hip with Displacement: From Case Studies to a Proposition for a Modified Diagnostic Path
- PMID: 35741282
- PMCID: PMC9222041
- DOI: 10.3390/diagnostics12061472
Secondary (Late) Developmental Dysplasia of the Hip with Displacement: From Case Studies to a Proposition for a Modified Diagnostic Path
Abstract
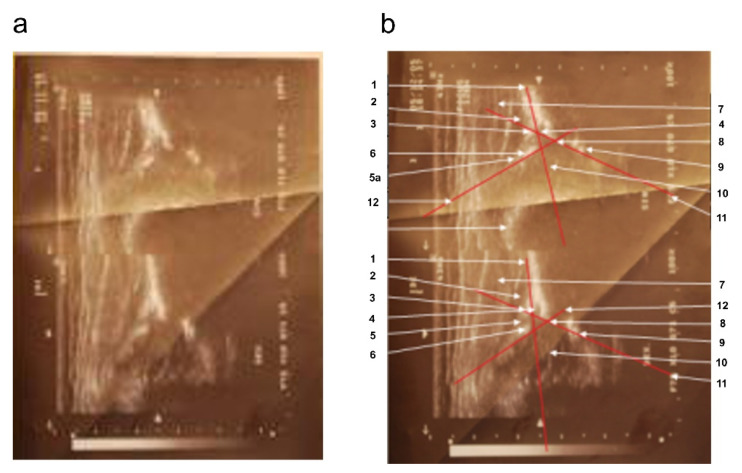
(1) Background. This paper presents a case of hip joints that were initially described as either normal or physiologically immature in four successive ultrasound examinations using the static method by Graf; however, the final treatment of the patient involved multiple hip reconstruction surgeries. (2) Case presentation. The patient was born with an Apgar score of 10 and did not exhibit neurological diseases that could deform and lead to pathological dislocation of the right hip joint. The subsequent analysis of medical data revealed that the hip luxation was due to secondary (late) developmental dysplasia of the right hip. (3) Conclusion. The article emphasizes the importance of early diagnosis and treatment standards for developmental dysplasia of the hip (DDH). The development of uniform international medical guidelines for the diagnosis, treatment, and prevention of hip dysplasia, along with the unification of DDH-related terminology, would allow for more effective management of DDH cases and reduce the cost of patient treatment.
Keywords: a case report of developmental dysplasia of the hip; diagnosis of dysplasia; treatment standards for developmental dysplasia of the hip.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Rehabilitacja medyczna. Tom 2, wyd. II. 2012. [(accessed on 27 December 2014)]. Available online: http://www.elsevier.pl/ksiazka/rehabilitacja-medyczna-tom-2-wyd-ii.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
