

Broadband Amplification as Tinnitus Treatment
- PMID: 35741602
- PMCID: PMC9221098
- DOI: 10.3390/brainsci12060719
Broadband Amplification as Tinnitus Treatment
Abstract
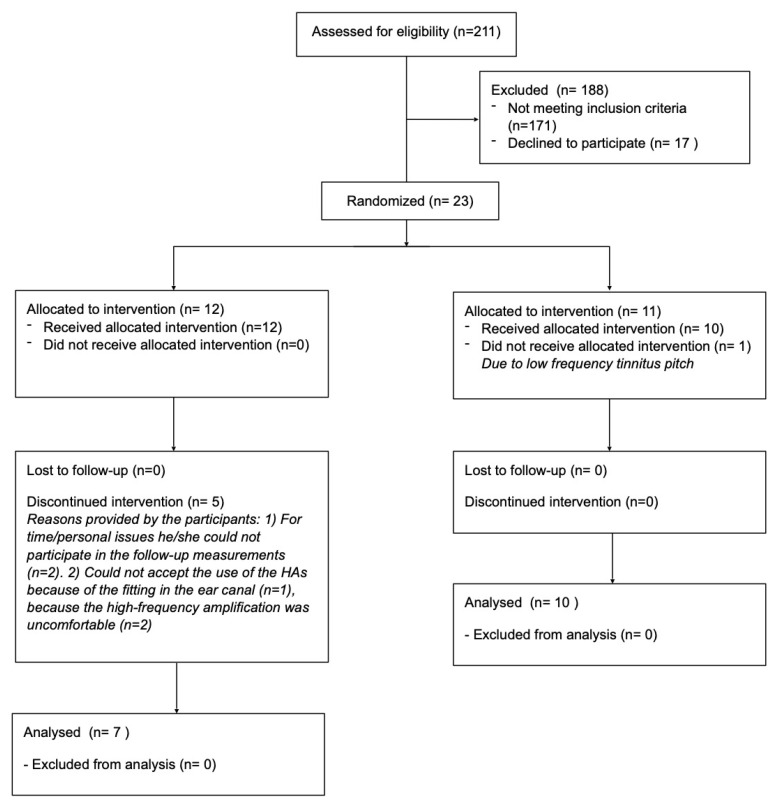
This study investigated the effect of broadband amplification (125 Hz to 10 kHz) as tinnitus treatment for participants with high-frequency hearing loss and compared these effects with an active placebo condition using band-limited amplification (125 Hz to 3-4 kHz). A double-blinded crossover study. Twenty-three participants with high-frequency (≥3 kHz) hearing loss and chronic tinnitus were included in the study, and 17 completed the full treatment protocol. Two different hearing aid treatments were provided for 3 months each: Broadband amplification provided gain in the frequency range from 125 Hz to 10 kHz and band-limited amplification only provided gain in the low-frequency range (≤3-4 kHz). The effect of the two treatments on tinnitus distress was evaluated with the Tinnitus Handicap Inventory (THI) and the Tinnitus Functional Index (TFI) questionnaires. The effect of the treatment on tinnitus loudness was evaluated with a visual analog scale (VAS) for loudness and a psychoacoustic loudness measure. Furthermore, the tinnitus annoyance was evaluated with a VAS for annoyance. The tinnitus pitch was evaluated based on the tinnitus likeness spectrum. A statistically significant difference was found between the two treatment groups (broadband vs. band-limited amplification) for the treatment-related change in THI and TFI with respect to the baseline. Furthermore, a statistically significant difference was found between the two treatment conditions for the annoyance measure. Regarding the loudness measure, no statistically significant differences were found between the treatments, although there was a trend towards a lower VAS-based loudness measure resulting from the broadband amplification. No changes were observed in the tinnitus pitch between the different conditions. Overall, the results from the present study suggest that tinnitus patients with high-frequency hearing loss can experience a decrease in tinnitus-related distress and annoyance from high-frequency amplification.
Keywords: amplification; hearing aids; high-frequency hearing loss; tinnitus.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures








References
Grants and funding
LinkOut - more resources
Full Text Sources
