

High Myoinositol on Proton MR Spectroscopy Could Be a Potential Signature of Papillary Tumors of the Pineal Region-Case Report of Two Patients
- PMID: 35741688
- PMCID: PMC9221252
- DOI: 10.3390/brainsci12060802
High Myoinositol on Proton MR Spectroscopy Could Be a Potential Signature of Papillary Tumors of the Pineal Region-Case Report of Two Patients
Abstract
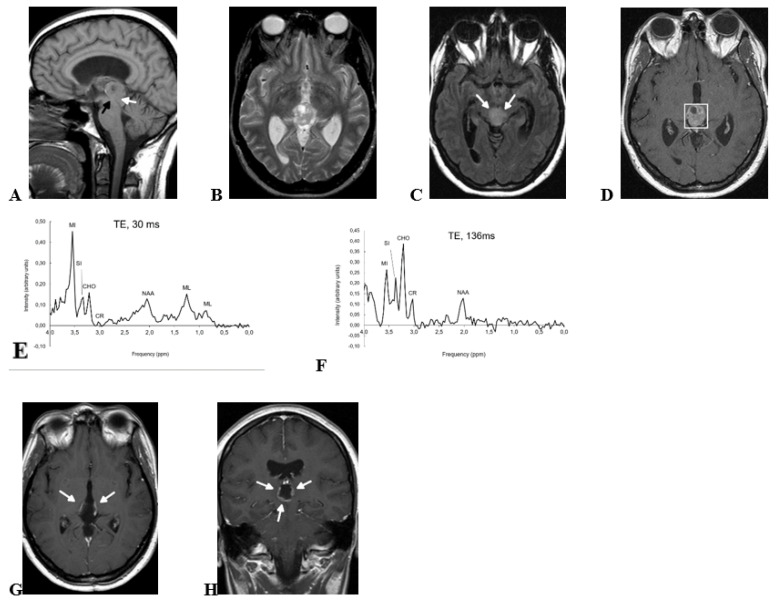
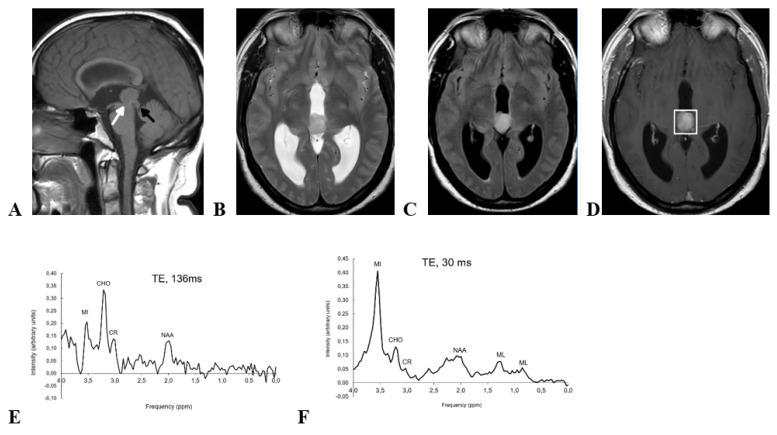
Papillary tumor of the pineal region (PTPR) is an uncommon entity in which a presurgical suspicion may be crucial for patient management. Maximal safe neurosurgical resection is of choice when PTPR is suspected, whereas non-surgical approaches can be considered in other tumors of the pineal region, such as pineocytoma or concrete subtypes of germ-cell tumors. In general terms, imaging features of tumors of the pineal region have been reported to be unspecific. Nevertheless, in this report, we describe two pathology-confirmed PTPRs in which presurgical proton MR spectroscopy demonstrated extremely high myoinositol, a pattern which drastically differs from that of other pineal tumors. We hypothesize that this high myoinositol may be related to PTPR's known ependymal component, and that it could be used as a specific non-invasive diagnostic signature.
Keywords: NMR spectroscopy; differential diagnosis; myoinositol; pineal neoplasms.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- WHO Classification of Tumours Editorial Board . World Health Organization Classification of Tumours of the Central Nervous System. 5th ed. International Agency for Research on Cancer; Lyon, France: 2021.
Publication types
LinkOut - more resources
Full Text Sources
