

Individual, Family, and Socioeconomic Contributors to Dental Caries in Children from Low- and Middle-Income Countries
- PMID: 35742362
- PMCID: PMC9222700
- DOI: 10.3390/ijerph19127114
Individual, Family, and Socioeconomic Contributors to Dental Caries in Children from Low- and Middle-Income Countries
Abstract
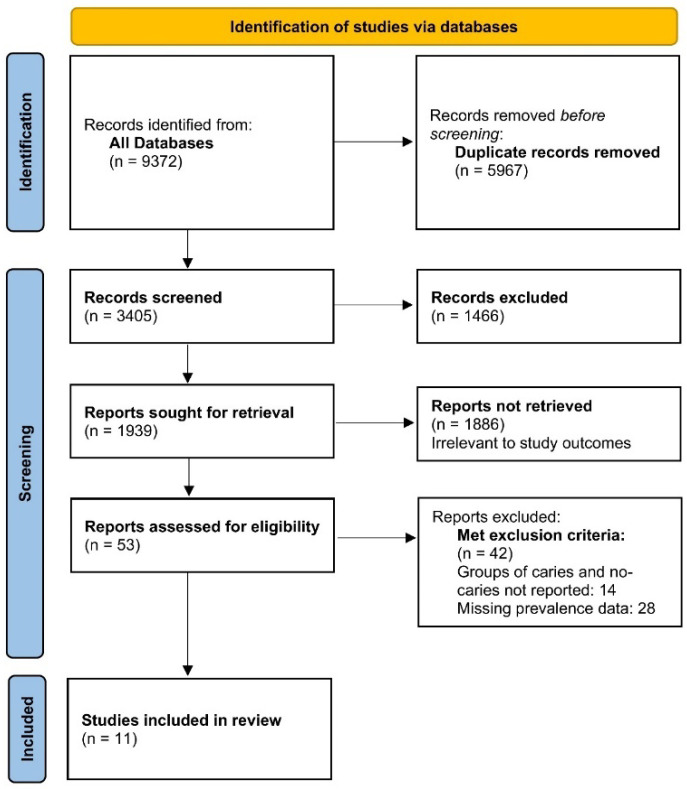
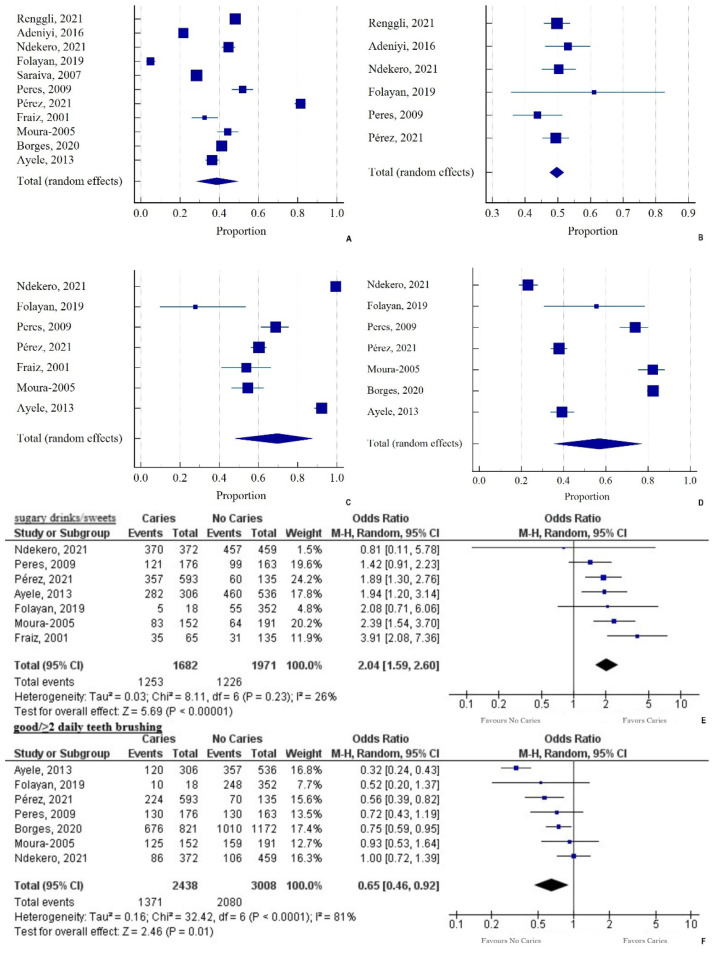
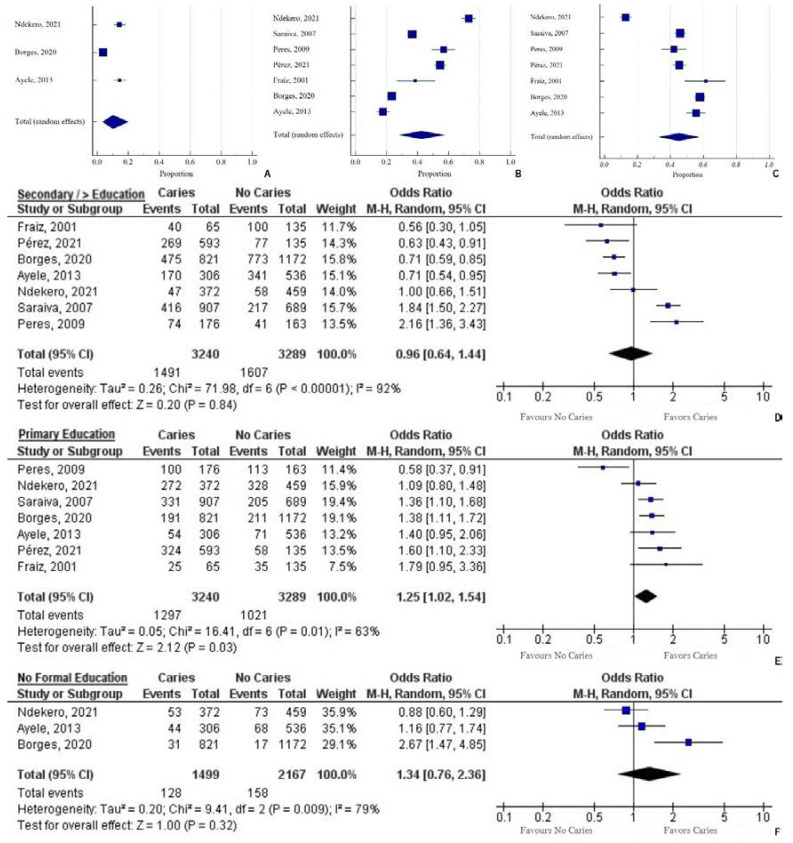
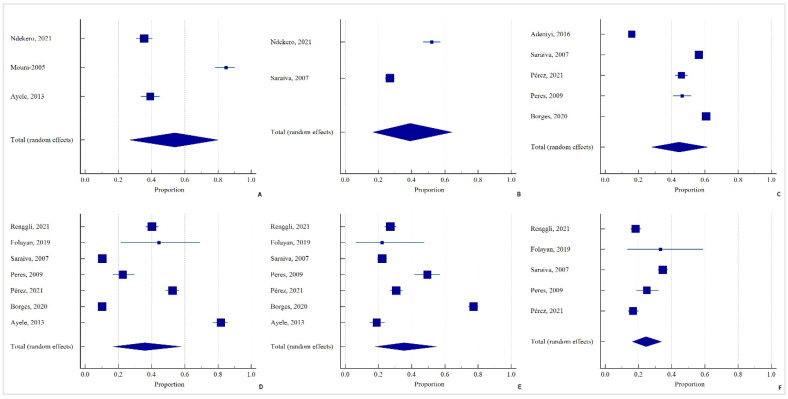
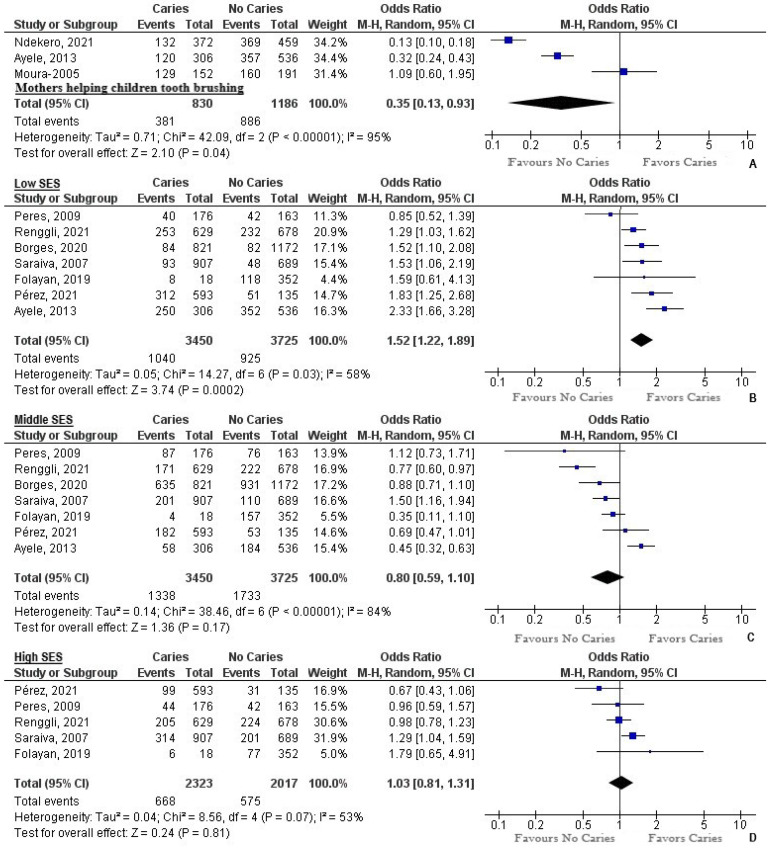
Introduction: Collective evidence on risk factors for dental caries remains elusive in low- and middle-income countries (LMICs). The objective was to conduct a systematic review and meta-analysis on risk factors for dental caries in deciduous or permanent teeth in LMICs. Methods: Studies were identified electronically through databases, including Cochrane Oral Health Group Trials Register, Cochrane Central Register of Controlled Trials, PubMed/MEDLINE, and CINAHL, using “prevalence, dental caries, child, family, socioeconomic, and LMIC” as the keywords. A total of 11 studies fit the inclusion criteria. Quality assessment of the included studies was performed using the Newcastle-Ottawa Scale (NOS). The MedCalc software and Review Manager 5.4.1 were used. Results: From 11,115 participants, 38.7% (95% CI: 28.4−49.5%) had caries and 49.68% were female. Among those with caries, 69.74% consumed sugary drinks/sweets (95% CI: 47.84−87.73%) and 56.87% (95% CI: 35.39−77.08%) had good brushing habits. Sugary drinks had a two times higher likelihood of leading to caries (OR: 2.04, p < 0.001). Good oral hygiene reduced the risk of caries by 35% (OR: 0.65, p < 0.001). Concerning maternal education, only secondary education reduced the likelihood of caries (OR: 0.96), but primary education incurred 25% higher risks (OR: 1.25, p = 0.03). A 65% reduction was computed when caregivers helped children with tooth brushing (OR: 0.35, p = 0.04). Most families had a low socioeconomic status (SES) (35.9%, 95% CI: 16.73−57.79), which increased the odds of caries by 52% (OR: 1.52, p < 0.001); a high SES had a 3% higher chance of caries. In the entire sample, 44.44% (95% CI: 27.73−61.82%) of individuals had access to dental services or had visited a dental service provider. Conclusion: Our findings demonstrate that high sugar consumption, low maternal education, and low and high socioeconomic status (SES) increased the risk of dental caries in LMICs. Good brushing habits, higher maternal education, help with tooth brushing, and middle SES provided protection against caries across LMIC children. Limiting sugars, improving oral health education, incorporating national fluoride exposure programs, and accounting for sociodemographic limitations are essential for reducing the prevalence of dental caries in these settings.
Keywords: bottle-feeding; breastfeeding; dental caries; education; fluoride; low- and middle-income countries; risk factors; socioeconomic status.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Sealants for preventing dental caries in primary teeth.Cochrane Database Syst Rev. 2022 Feb 11;2(2):CD012981. doi: 10.1002/14651858.CD012981.pub2. Cochrane Database Syst Rev. 2022. PMID: 35146744 Free PMC article.
-
Slow-release fluoride devices for the control of dental decay.Cochrane Database Syst Rev. 2018 Mar 1;3(3):CD005101. doi: 10.1002/14651858.CD005101.pub4. Cochrane Database Syst Rev. 2018. PMID: 29495063 Free PMC article.
-
Direct composite resin fillings versus amalgam fillings for permanent posterior teeth.Cochrane Database Syst Rev. 2021 Aug 13;8(8):CD005620. doi: 10.1002/14651858.CD005620.pub3. Cochrane Database Syst Rev. 2021. PMID: 34387873 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Pulp treatment for extensive decay in primary teeth.Cochrane Database Syst Rev. 2018 May 31;5(5):CD003220. doi: 10.1002/14651858.CD003220.pub3. Cochrane Database Syst Rev. 2018. PMID: 29852056 Free PMC article.
Cited by
-
Activity and levels of TNF-α, IL-6 and IL-8 in saliva of children and young adults with dental caries: a systematic review and meta-analysis.BMC Oral Health. 2024 Jul 18;24(1):816. doi: 10.1186/s12903-024-04560-8. BMC Oral Health. 2024. PMID: 39026257 Free PMC article.
-
Applications of AI-based deep learning models for detecting dental caries on intraoral images - a systematic review.Evid Based Dent. 2025 Mar;26(1):71-72. doi: 10.1038/s41432-024-01089-1. Epub 2024 Nov 28. Evid Based Dent. 2025. PMID: 39609513
-
The effect of unhealthy dietary habits on the incidence of dental caries and overweight/obesity among Egyptian school children (A cross-sectional study).Front Public Health. 2022 Aug 16;10:953545. doi: 10.3389/fpubh.2022.953545. eCollection 2022. Front Public Health. 2022. PMID: 36052005 Free PMC article.
-
Dental caries and actual utilization of dental services among primary school children in Egypt: a cross-sectional study.BMC Oral Health. 2025 Jul 15;25(1):1163. doi: 10.1186/s12903-025-06414-3. BMC Oral Health. 2025. PMID: 40665234 Free PMC article.
-
Microinvasive interventions in the management of proximal caries lesions in primary and permanent teeth- systematic review and meta-analysis.BMC Oral Health. 2025 Jan 8;25(1):48. doi: 10.1186/s12903-024-05400-5. BMC Oral Health. 2025. PMID: 39780151 Free PMC article.
References
-
- Kassebaum N.J., Smith A.G.C., Bernabé E., Fleming T.D., Reynolds A.E., Vos T., Murray C.J.L., Marcenes W., GBD Oral Health Collaborators Global, Regional, and National Prevalence, Incidence, and Disability-Adjusted Life Years for Oral Conditions for 195 Countries, 1990–2015: A Systematic Analysis for the Global Burden of Diseases, Injuries, and Risk Factors. J. Dent. Res. 2017;96:380–387. doi: 10.1177/0022034517693566. - DOI - PMC - PubMed
-
- El Tantawi M., Folayan M.O., Mehaina M., Vukovic A., Castillo J.L., Gaffar B.O., Arheiam A., Al-Batayneh O.B., Kemoli A.M., Schroth R.J. Prevalence and Data Availability of Early Childhood Caries in 193 United Nations Countries, 2007–2017. Am. J. Public Health. 2018;108:1066–1072. doi: 10.2105/AJPH.2018.304466. - DOI - PMC - PubMed
-
- Mathu-Muju K.R., Friedman J.W., Nash D.A. Oral Health Care for Children in Countries Using Dental Therapists in Public, School-Based Programs, Contrasted with That of the United States, Using Dentists in a Private Practice Model. Am. J. Public Health. 2013;103:e7–e13. doi: 10.2105/AJPH.2013.301251. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
