

Uterine Septum with or without Hysteroscopic Metroplasty: Impact on Fertility and Obstetrical Outcomes-A Systematic Review and Meta-Analysis of Observational Research
- PMID: 35743362
- PMCID: PMC9224595
- DOI: 10.3390/jcm11123290
Uterine Septum with or without Hysteroscopic Metroplasty: Impact on Fertility and Obstetrical Outcomes-A Systematic Review and Meta-Analysis of Observational Research
Abstract
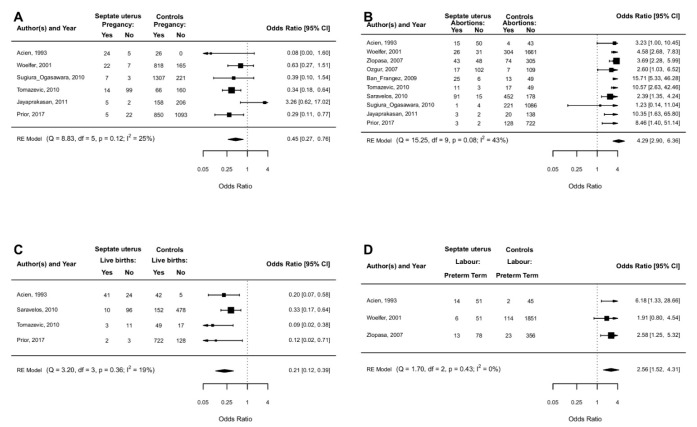
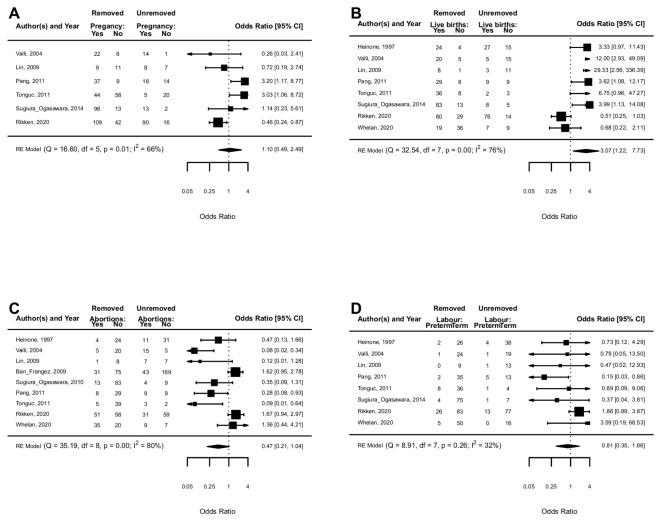
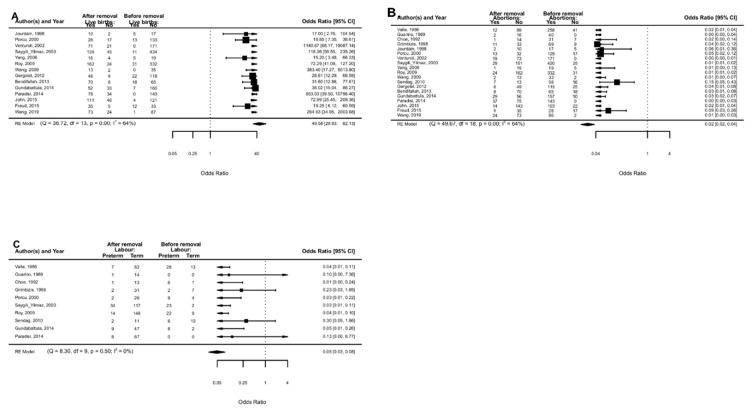
Objective: we performed a systematic review/meta-analysis to evaluate the impact of septate uterus and hysteroscopic metroplasty on pregnancy rate-(PR), live birth rate-(LBR), spontaneous abortion-(SA) and preterm labor (PL) in infertile/recurrent miscarriage-(RM) patients. Data sources: a literature search of relevant papers was conducted using electronic bibliographic databases (Medline, Scopus, Embase, Science direct). Study eligibility criteria: we included in this meta-analysis all types of observational studies that evaluated the clinical impact of the uterine septum and its resection (hysteroscopic metroplasty) on reproductive and obstetrics outcomes. The population included were patients with a diagnosis of infertility or recurrent pregnancy loss. Study appraisal and synthesis methods: outcomes were evaluated according to three subgroups: (i) Women with untreated uterine septum versus women without septum (controls); (ii) Women with treated uterine septum versus women with untreated septum (controls); (iii) Women before and after septum removal. Odds ratios (OR) with 95% confidence intervals (CI) were calculated for the outcome measures. A p-value < 0.05 was considered statistically significant. Subgroup analysis was performed according to the depth of the septum. Sources of heterogeneity were explored by meta-regression analysis according to specific features: assisted reproductive technology/spontaneous conception, study design and quality of papers included Results: data from 38 studies were extracted. (i) septum versus no septum: a lower PR and LBR were associated with septate uterus vs. controls (OR 0.45, 95% CI 0.27−0.76; p < 0.0001; and OR 0.21, 95% CI 0.12−0.39; p < 0.0001); a higher proportion of SA and PL was associated with septate uterus vs. controls (OR 4.29, 95% CI 2.90−6.36; p < 0.0001; OR 2.56, 95% CI 1.52−4.31; p = 0.0004). (ii) treated versus untreated septum: PR and PL were not different in removed vs. unremoved septum(OR 1.10, 95% CI 0.49−2.49; p = 0.82 and OR 0.81, 95% CI 0.35−1.86; p = 0.62); a lower proportion of SA was associated with removed vs. unremoved septum (OR 0.47, 95% CI 0.21−1.04; p = 0.001); (iii) before-after septum removal: the proportion of LBR was higher after the removal of septum (OR 49.58, 95% CI 29.93−82.13; p < 0.0001) and the proportion of SA and PL was lower after the removal of the septum (OR 0.02, 95% CI 0.02−0.04; p < 0.000 and OR 0.05, 95% CI 0.03−0.08; p < 0.0001) Conclusions: the results show the detrimental effect of the uterine septum on PR, LBR, SA and PL. Its treatment reduces the rate of SA.
Keywords: infertility; live birth rate; metroplasty; pregnancy rate; preterm labour; recurrent miscarriage; spontaneous abortion; uterine septum.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Acien P., Acien M. Evidence-based management of recurrent miscarriage. Surg. Manag. 2004;1:335–342.
-
- American Fertility Society The American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, müllerian anomalies and intrauterine adhesions. Fertil. Steril. 1988;49:944–955. doi: 10.1016/S0015-0282(16)59942-7. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
