

Fetal Brain Development: Regulating Processes and Related Malformations
- PMID: 35743840
- PMCID: PMC9224903
- DOI: 10.3390/life12060809
Fetal Brain Development: Regulating Processes and Related Malformations
Abstract
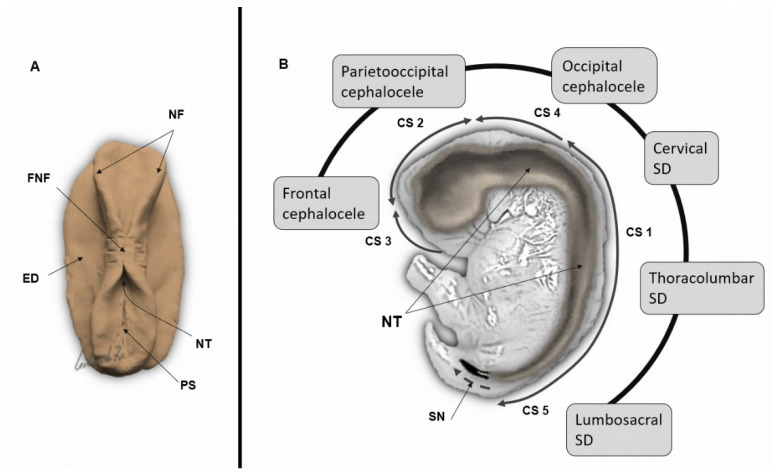
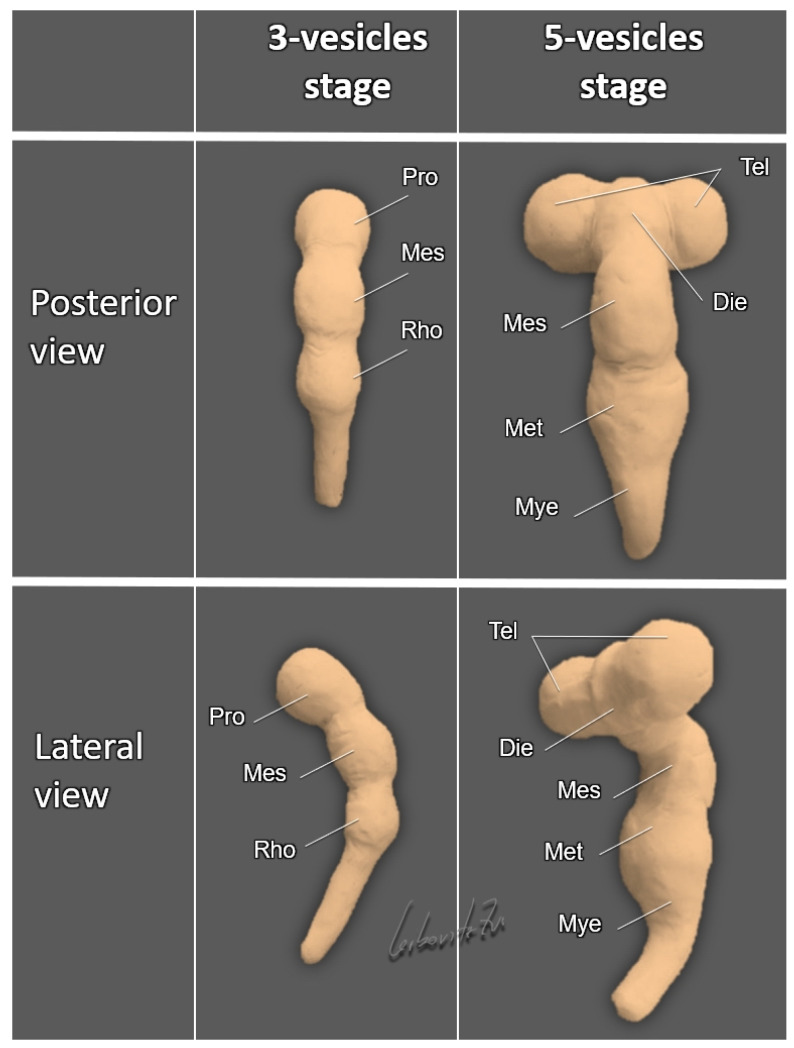
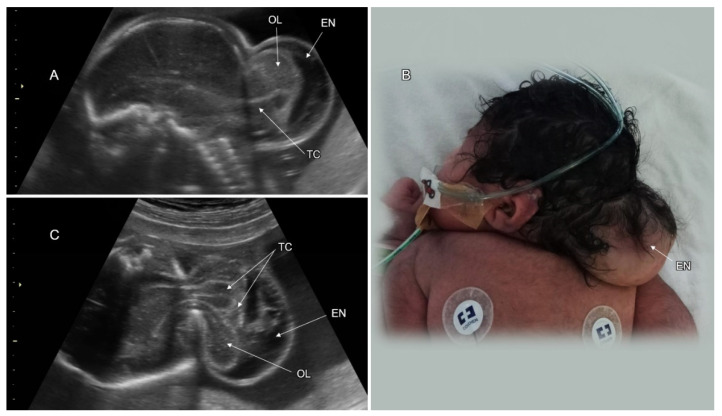
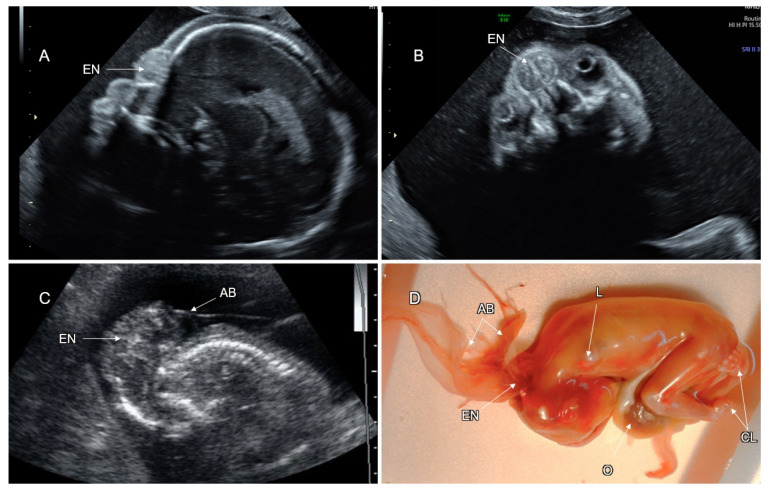
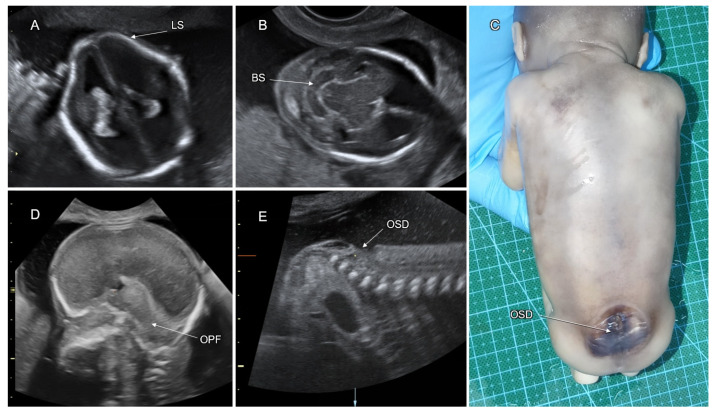
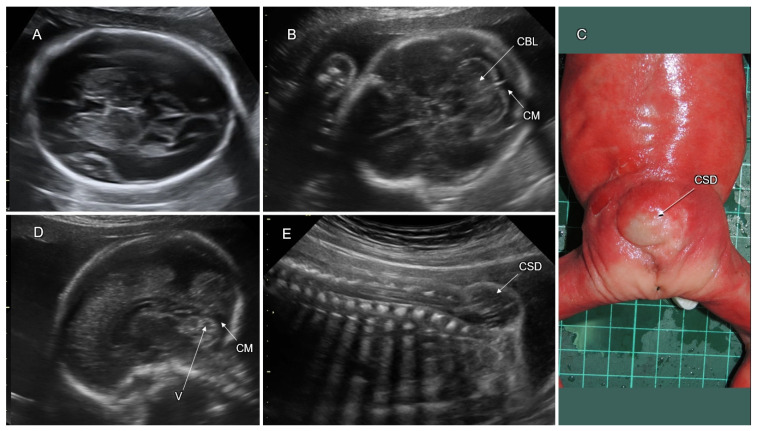
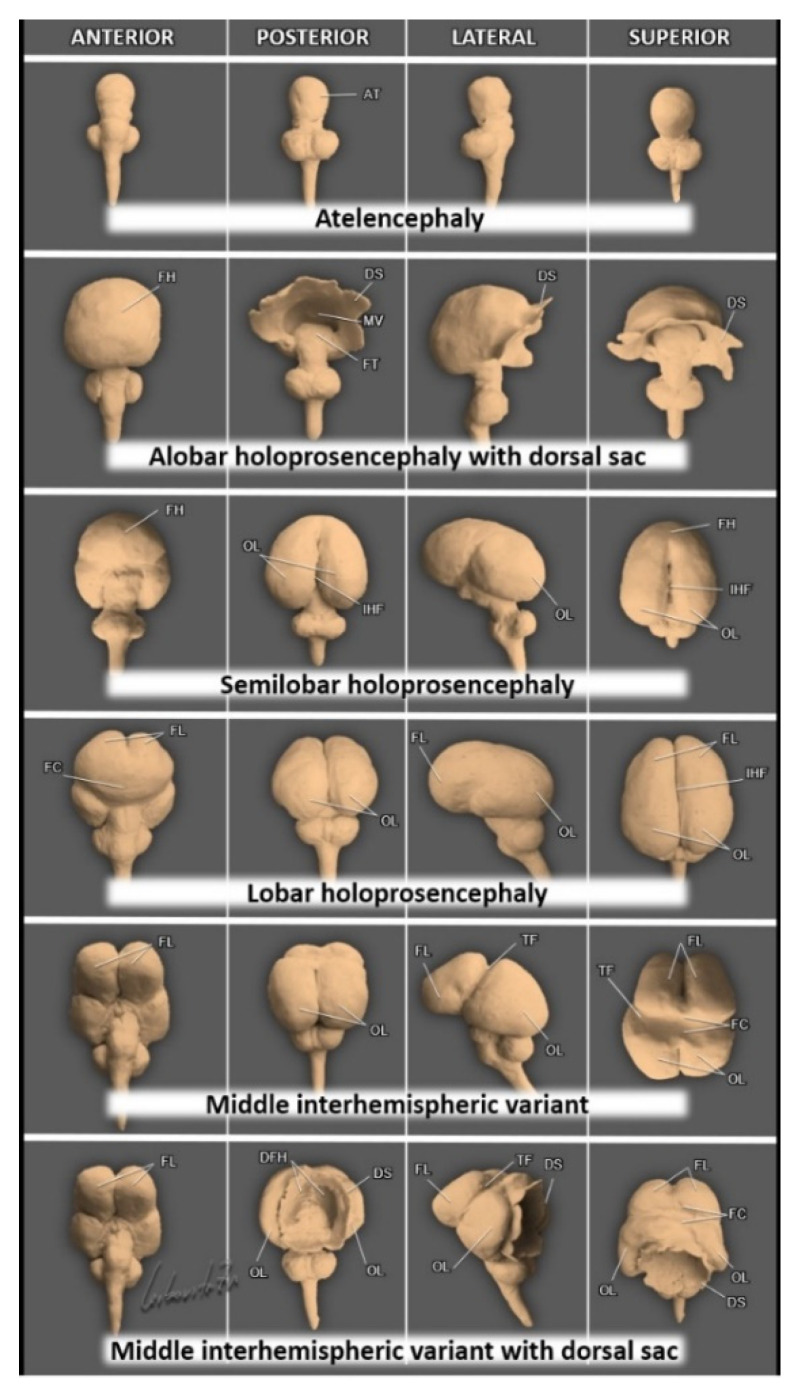
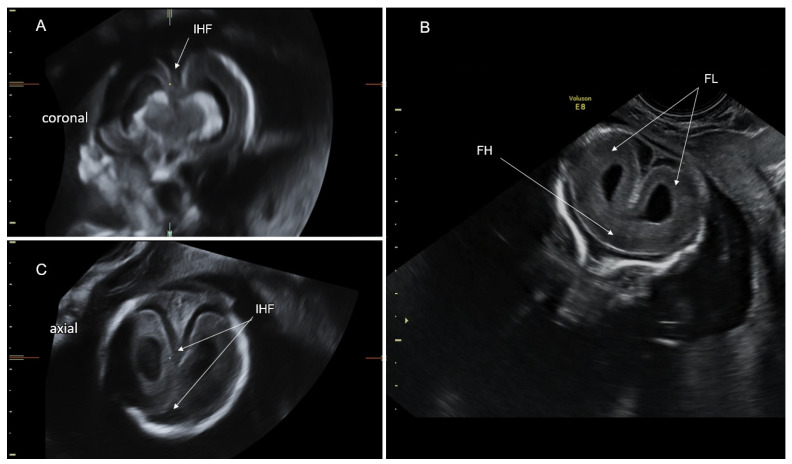
This paper describes the contemporary state of knowledge regarding processes that regulate normal development of the embryonic-fetal central nervous system (CNS). The processes are described according to the developmental timetable: dorsal induction, ventral induction, neurogenesis, neuronal migration, post-migration neuronal development, and cortical organization. We review the current literature on CNS malformations associated with these regulating processes. We specifically address neural tube defects, holoprosencephaly, malformations of cortical development (including microcephaly, megalencephaly, lissencephaly, cobblestone malformations, gray matter heterotopia, and polymicrogyria), disorders of the corpus callosum, and posterior fossa malformations. Fetal ventriculomegaly, which frequently accompanies these disorders, is also reviewed. Each malformation is described with reference to the etiology, genetic causes, prenatal sonographic imaging, associated anomalies, differential diagnosis, complimentary diagnostic studies, clinical interventions, neurodevelopmental outcome, and life quality.
Keywords: CNS malformations; brain development; fetal neurology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures






References
-
- Van Allen M.I. Multisite neural tube closure in humans. Birth Defects Orig. Artic. Ser. 1996;30:203–225. - PubMed
-
- ten Donkelaar H., van der Vliet T. Overview of the Development of the Human Brain and Spinal Cord. In: ten Donkelaar H., Lammens M., editors. Clinical Neuroembryology. 1st ed. Springer; Würzburg, Germany: 2006. pp. 1–40.
Publication types
LinkOut - more resources
Full Text Sources
