

Hypofractionation and Concomitant Boost in Ductal Carcinoma In Situ (DCIS): Analysis of a Prospective Case Series with Long-Term Follow-Up
- PMID: 35743920
- PMCID: PMC9225308
- DOI: 10.3390/life12060889
Hypofractionation and Concomitant Boost in Ductal Carcinoma In Situ (DCIS): Analysis of a Prospective Case Series with Long-Term Follow-Up
Abstract
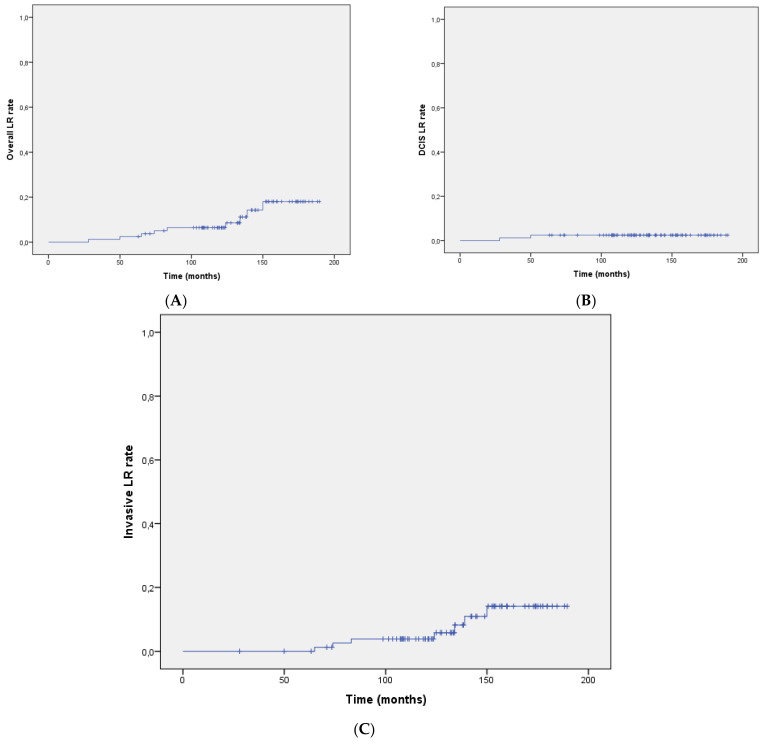
We previously reported on a cohort of breast cancer patients affected with ductal carcinoma in situ (DCIS) that were treated with breast conservative surgery and hypofractionated whole-breast radiotherapy with a concomitant boost to the lumpectomy cavity. We now report on the long-term results of the oncological and toxicity outcomes, at a median follow-up of 11.2 years. We also include an analysis of the predictive factors for local recurrence (LR). Eighty-two patients with long-term observation were considered for this report. All received hypofractionated post-operative radiotherapy with a concomitant boost (45 Gy/20 fractions to the whole breast and 50 Gy/20 fractions to the lumpectomy cavity). We report on LC rates at 5 and 10 years, overall survival (OS), and breast-cancer-specific survival (BCSS), employing the Kaplan-Meier method. Cox proportional regression analysis was used to determine the role of selected clinical parameters on the risk of local recurrence, by the univariate and multivariate models. After a median follow-up of 11.2 years (range 5-15 years), 9 pts (11%) developed LR. The LR rates at 5 years and 10 years were 2.4% and 8.2%, respectively. The 5- and 10-year overall survival rates were 98.8% and 91.6%, respectively. The 5- and 10-year breast-cancer-specific survival rates were 100.0% and 99.0%. Late skin and subcutaneous toxicities were generally mild, and cosmetic results were good-excellent for most patients. For the univariate regression analysis, ER positive status (HR; 95% CI, p = 0.021), PgR positive status (HR; 95% CI, p = 0.012), and the aggregate data of positive hormonal status (HR; 95% CI, p = 0.021) were inversely correlated to LR risk. Conversely, a high tumor grade (G3) was directly correlated with the risk of LR (HR; 95% CI, p = 0.048). For the multivariate regression analysis, a high tumor grade (G3) confirmed its negative impact on LR (HR 0.40; 95% CI 0.19-0.75, p = 0.047). Our long-term data demonstrate hypofractionated whole-breast radiotherapy with a concomitant boost to be feasable, effective, and tolerable. Our experience suggests positive hormonal status to be protective with respect to LR risk. A high tumor grade is a risk factor for LR.
Keywords: DCIS; ductal carcinoma in situ; hypofractionated radiotherapy; hypofractionation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



References
-
- DeSnyder S.M., Hunt K.K., Dong W., Smith B.D., Moran M.S., Mac Gregor M.C., Shen Y., Kuerer H.M., Lucci A. American Society of Breast Surgeons’ practice patterns after publication of the SSO-ASTRO-ASCO DCIS consensus guideline on margins from breast-conserving surgery with whole-breast irradiation. Ann. Surg. Oncol. 2018;25:2965–2974. doi: 10.1245/s10434-018-6580-9. - DOI - PubMed
-
- McCormick B., Winter K., Hudis C., Kuerer H.M., Rakovitch E., Smith B.L., Sneige N., Moughan J., Shah A., Germain I., et al. RTOG 9804: A prospective randomized trial for good-risk ductal carcinoma in situ comparing radiotherapy with observation. J. Clin. Oncol. 2015;33:709–715. doi: 10.1200/JCO.2014.57.9029. - DOI - PMC - PubMed
-
- Offersen B.V., Alsner J., Nielsen H.M., Jakobsen E.H., Nielsen M.H., Krause M., Stenbygaard L., Mjaaland I., Schreiber A., Kasti U.-M., et al. Hypofractionated versus standard fractionated radiotherapy in patients with early breast cancer or ductal carcinoma in situ in a randomized phase III trial: The DBCG HYPO trial. J. Clin. Oncol. 2020;38:3615–3625. doi: 10.1200/JCO.20.01363. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
