

SARS-CoV-2 Infection Is Associated with Uncontrolled HIV Viral Load in Non-Hospitalized HIV-Infected Patients from Gugulethu, South Africa
- PMID: 35746693
- PMCID: PMC9229655
- DOI: 10.3390/v14061222
SARS-CoV-2 Infection Is Associated with Uncontrolled HIV Viral Load in Non-Hospitalized HIV-Infected Patients from Gugulethu, South Africa
Abstract
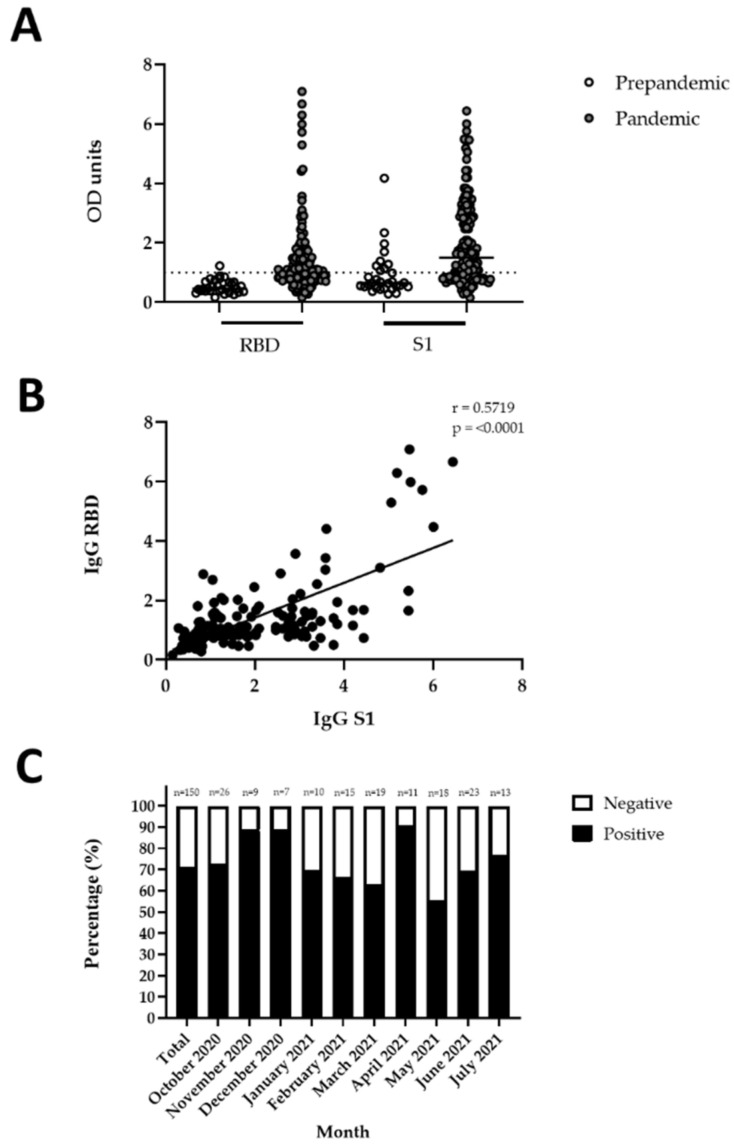
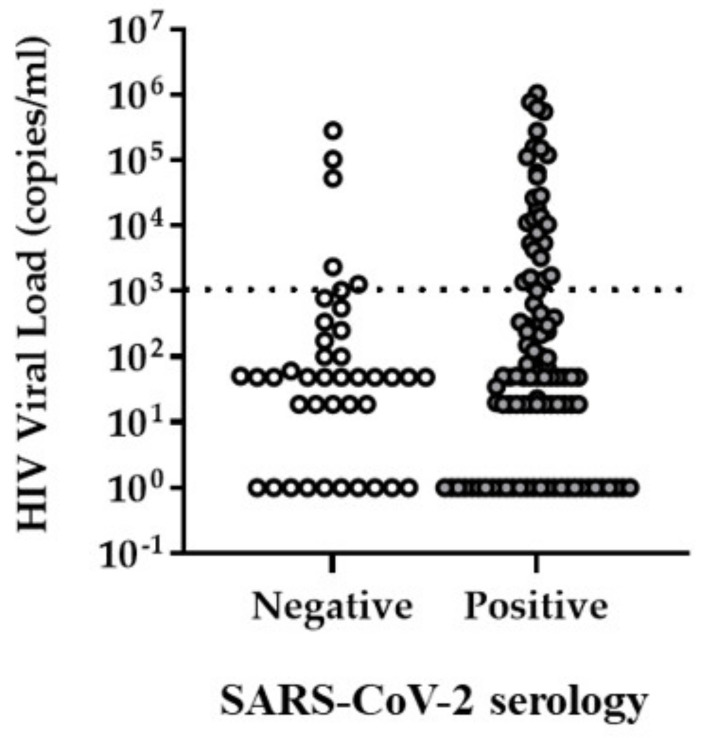
In South Africa, high exposure to SARS-CoV-2 occurs primarily in densely populated, low-income communities, which are additionally burdened by highly prevalent Human Immunodeficiency Virus (HIV). With the aim to assess SARS-CoV-2 seroprevalence and its association with HIV-related clinical parameters in non-hospitalized patients likely to be highly exposed to SARS-CoV-2, this observational cross-sectional study was conducted at the Gugulethu Community Health Centre Antiretroviral clinic between October 2020 and June 2021, after the first COVID-19 wave in South Africa and during the second and beginning of the third wave. A total of 150 adult (median age 39 years [range 20−65 years]) HIV-infected patients (69% female; 31% male) were recruited. 95.3% of the cohort was on antiretroviral therapy (ART), had a median CD4 count of 220 cells/µL (range 17−604 cells/µL) and a median HIV viral load (VL) of 49 copies/mL (range 1−1,050,867 copies/mL). Furthermore, 106 patients (70.7%) were SARS-CoV-2 seropositive, and 0% were vaccinated. When stratified for HIV VL, patients with uncontrolled HIV viremia (HIV VL > 1000 copies/mL) had significantly higher odds of SARS-CoV-2 seropositivity than patients with HIV VL < 1000 copies/mL, after adjusting for age, sex and ART status (p = 0.035, adjusted OR 2.961 [95% CI: 1.078−8.133]). Although the cause−effect relationship could not be determined due to the cross-sectional study design, these results point towards a higher risk of SARS-CoV-2 susceptibility among viremic HIV patients, or impaired HIV viral control due to previous co-infection with SARS-CoV-2.
Keywords: ART; COVID-19; HIV; PLWH; SARS-CoV-2; South Africa; viral load.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- UNAIDS. Country Factsheet South Africa 2020. [(accessed on 2 March 2022)]. Available online: https://www.unaids.org/en/regionscountries/countries/southafrica.
-
- Adams J., MacKenzie M.J., Amegah A.K., Ezeh A., Gadanya M.A., Omigbodun A., Sarki A.M., Thistle P., Ziraba A.K., Stranges S., et al. The Conundrum of Low COVID-19 Mortality Burden in sub-Saharan Africa: Myth or Reality? Glob. Health Sci. Pract. 2021;9:433–443. doi: 10.9745/GHSP-D-21-00172. - DOI - PMC - PubMed
-
- MRC. Report on Weekly Deaths in South Africa. [(accessed on 11 April 2022)]. Available online: https://www.samrc.ac.za/reports/report-weekly-deaths-south-africa?bc=254.
-
- Jassat W., Cohen C., Tempia S., Masha M., Goldstein S., Kufa T., Murangandi P., Savulescu D., Walaza S., Bam J.L., et al. Risk factors for COVID-19-related in-hospital mortality in a high HIV and tuberculosis prevalence setting in South Africa: A cohort study. Lancet HIV. 2021;8:e554–e567. doi: 10.1016/S2352-3018(21)00151-X. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
