

High and Sustained Ex Vivo Frequency but Altered Phenotype of SARS-CoV-2-Specific CD4+ T-Cells in an Anti-CD20-Treated Patient with Prolonged COVID-19
- PMID: 35746736
- PMCID: PMC9228841
- DOI: 10.3390/v14061265
High and Sustained Ex Vivo Frequency but Altered Phenotype of SARS-CoV-2-Specific CD4+ T-Cells in an Anti-CD20-Treated Patient with Prolonged COVID-19
Abstract
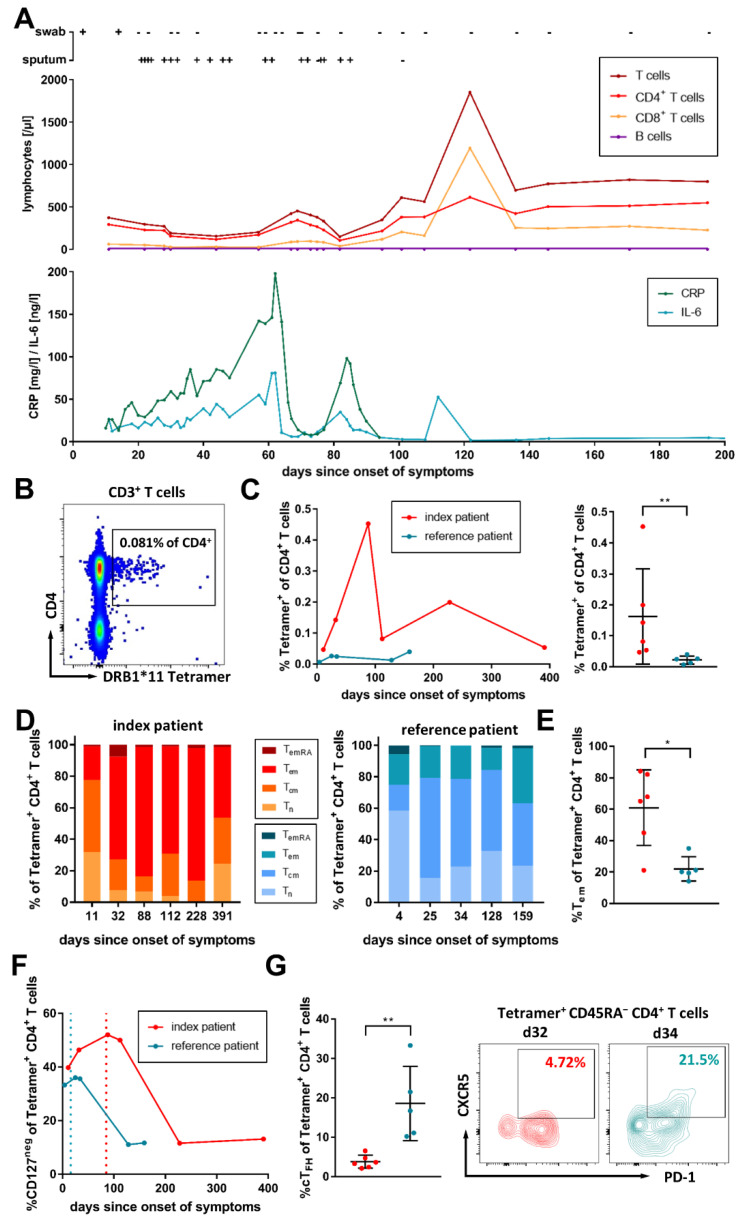
Here, we longitudinally assessed the ex vivo frequency and phenotype of SARS-CoV-2 membrane protein (aa145-164) epitope-specific CD4+ T-cells of an anti-CD20-treated patient with prolonged viral positivity in direct comparison to an immunocompetent patient through an MHC class II DRB1*11:01 Tetramer analysis. We detected a high and stable SARS-CoV-2 membrane-specific CD4+ T-cell response in both patients, with higher frequencies of virus-specific CD4+ T-cells in the B-cell-depleted patient. However, we found an altered virus-specific CD4+ T-cell memory phenotype in the B-cell-depleted patient that was skewed towards late differentiated memory T-cells, as well as reduced frequencies of SARS-CoV-2-specific CD4+ T-cells with CD45RA- CXCR5+ PD-1+ circulating T follicular helper cell (cTFH) phenotype. Furthermore, we observed a delayed contraction of CD127- virus-specific effector cells. The expression of the co-inhibitory receptors TIGIT and LAG-3 fluctuated on the virus-specific CD4+ T-cells of the patient, but were associated with the inflammation markers IL-6 and CRP. Our findings indicate that, despite B-cell depletion and a lack of B-cell-T-cell interaction, a robust virus-specific CD4+ T-cell response can be primed that helps to control the viral replication, but which is not sufficient to fully abrogate the infection.
Keywords: CD39; CD4+ T-cells; CD73; COVID-19; MHC class II Tetramer; PD-1; SARS-CoV-2; T-cell memory; TIGIT; anti-CD20 therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Andersen K.M., Bates B.A., Rashidi E.S., Olex A.L., Mannon R.B., Patel R.C., Singh J., Sun J., Auwaerter P.G., Ng D.K., et al. Long-term use of immunosuppressive medicines and in-hospital COVID-19 outcomes: A retrospective cohort study using data from the National COVID Cohort Collaborative. Lancet Rheumatol. 2022;4:e33–e41. doi: 10.1016/S2665-9913(21)00325-8. - DOI - PMC - PubMed
-
- Weigang S., Fuchs J., Zimmer G., Schnepf D., Kern L., Beer J., Luxenburger H., Ankerhold J., Falcone V., Kemming J., et al. Within-host evolution of SARS-CoV-2 in an immunosuppressed COVID-19 patient as a source of immune escape variants. Nat. Commun. 2021;12:6405. doi: 10.1038/s41467-021-26602-3. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
