

Evaluation of Screening Program and Phylogenetic Analysis of SARS-CoV-2 Infections among Hospital Healthcare Workers in Liège, Belgium
- PMID: 35746774
- PMCID: PMC9227503
- DOI: 10.3390/v14061302
Evaluation of Screening Program and Phylogenetic Analysis of SARS-CoV-2 Infections among Hospital Healthcare Workers in Liège, Belgium
Abstract
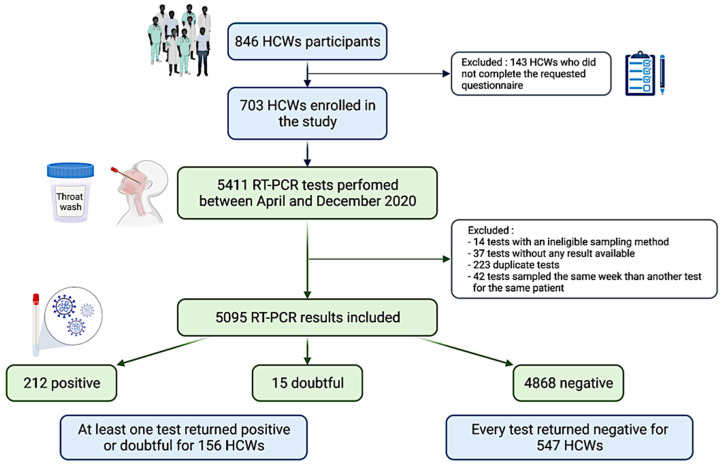
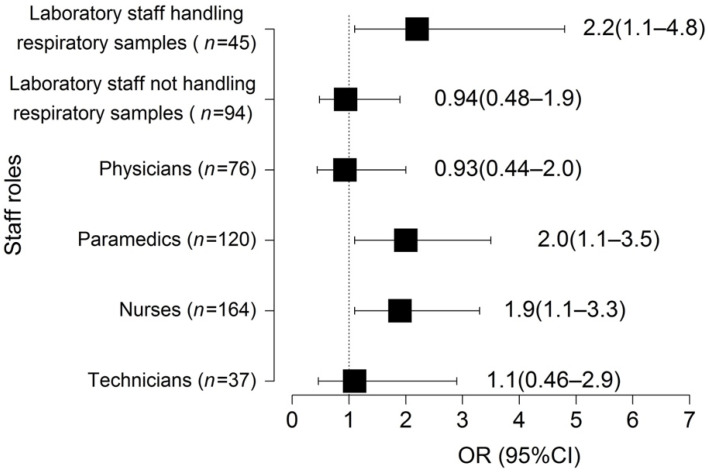
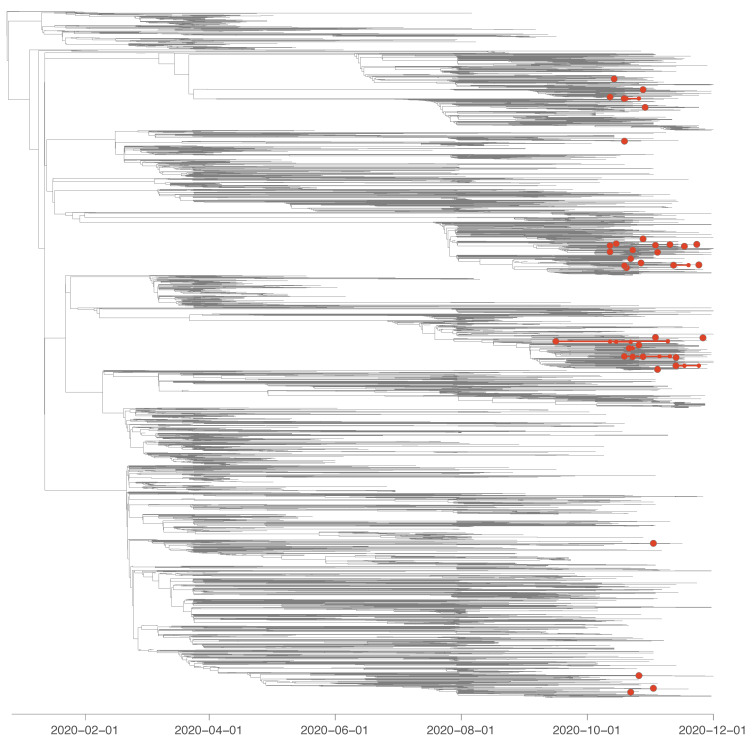
Healthcare workers (HCWs) are known to be at higher risk of developing severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infections although whether these risks are equal across all occupational roles is uncertain. Identifying these risk factors and understand SARS-CoV-2 transmission pathways in healthcare settings are of high importance to achieve optimal protection measures. We aimed to investigate the implementation of a voluntary screening program for SARS-CoV-2 infections among hospital HCWs and to elucidate potential transmission pathways though phylogenetic analysis before the vaccination era. HCWs of the University Hospital of Liège, Belgium, were invited to participate in voluntary reverse transcriptase-polymerase chain reaction (RT-PCR) assays performed every week from April to December 2020. Phylogenetic analysis of SARS-CoV-2 genomes were performed for a subgroup of 45 HCWs. 5095 samples were collected from 703 HCWs. 212 test results were positive, 15 were indeterminate, and 4868 returned negative. 156 HCWs (22.2%) tested positive at least once during the study period. All SARS-CoV-2 test results returned negative for 547 HCWs (77.8%). Nurses (p < 0.05), paramedics (p < 0.05), and laboratory staff handling respiratory samples (p < 0.01) were at higher risk for being infected compared to the control non-patient facing group. Our phylogenetic analysis revealed that most positive samples corresponded to independent introduction events into the hospital. Our findings add to the growing evidence of differential risks of being infected among HCWs and support the need to implement appropriate protection measures based on each individual’s risk profile to guarantee the protection of both HCWs and patients. Furthermore, our phylogenetic investigations highlight that most positive samples correspond to distinct introduction events into the hospital.
Keywords: COVID-19; SARS-CoV-2; healthcare workers; healthcare-associated transmission; infection prevention and control; occupational exposure; phylogenetic analysis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- COVID-19 Surveillance Frequently Asked Questions. Sciensano. [(accessed on 20 December 2021)]. Available online: https://covid19.sciensano.be/sites/default/files/Covid19/COVID-19_FAQ_EN....
-
- Meurisse M., Lajot A., Dupont Y., Lesenfants M., Klamer S., Rebolledo J., Lernout T., Leroy M., Capron A., Van Bussel J., et al. One year of laboratory-based COVID-19 surveillance system in Belgium: Main indicators and performance of the laboratories. Arch. Belg. Public Health. 2021;79:188. doi: 10.1186/s13690-021-00704-2. - DOI - PMC - PubMed
-
- Iversen K., Bundgaard H., Hasselbalch R.B., Kristensen J.H., Nielsen P.B., Pries-Heje M., Knudsen A.D., Christensen C.E., Fogh K., Norsk J.B., et al. Risk of COVID-19 in health-care workers in Denmark: An observational cohort study. Lancet Infect. Dis. 2020;20:1401–1408. doi: 10.1016/S1473-3099(20)30589-2. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
