

Prospective associations of health literacy with clinical outcomes in adults with CKD: findings from the CRIC study
- PMID: 35746879
- PMCID: PMC10064835
- DOI: 10.1093/ndt/gfac201
Prospective associations of health literacy with clinical outcomes in adults with CKD: findings from the CRIC study
Abstract
Background: Limited health literacy is associated with significant morbidity and mortality in the general population but the relation of health literacy with long-term clinical outcomes among adults with chronic kidney disease (CKD) is less clear.
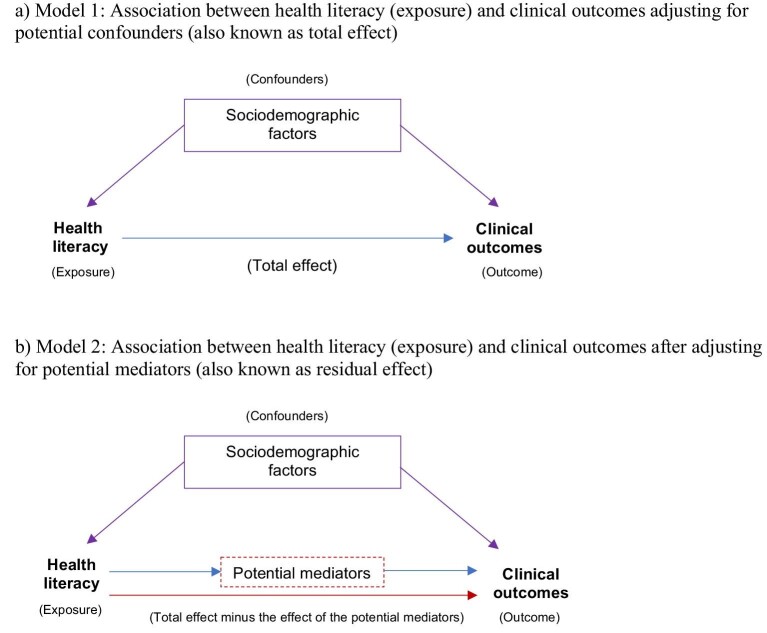
Methods: Prospective data from the Chronic Renal Insufficiency Cohort (CRIC) Study (n = 3715) were used. Health literacy was assessed with the Short Test of Functional Health Literacy in Adults (dichotomized as limited/adequate). Cox proportional hazards models were used to separately examine the relations of health literacy with CKD progression, cardiovascular event (any of the following: myocardial infarction, congestive heart failure, stroke or peripheral artery disease), and all-cause, cardiovascular and non-cardiovascular mortality. Poisson regression was used to assess the health literacy-hospitalization association. Models were sequentially adjusted: Model 1 adjusted for potential confounders (sociodemographic factors), while Model 2 additionally adjusted for potential mediators (clinical and lifestyle factors) of the associations of interest.
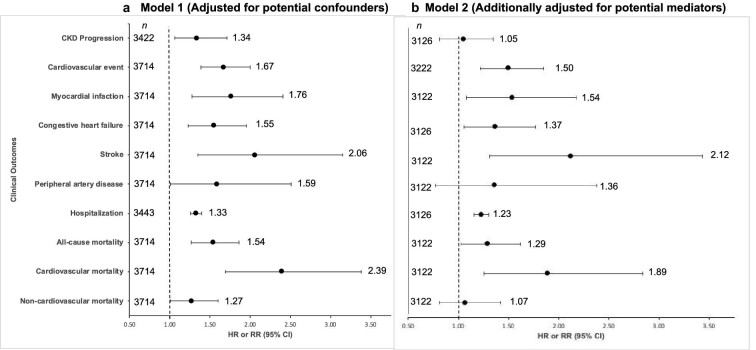
Results: In confounder-adjusted models, participants with limited (vs adequate) health literacy [555 (15%)] had an increased risk of CKD progression [hazard ratio (HR) 1.34; 95% confidence interval (CI) 1.06-1.71], cardiovascular event (HR 1.67; 95% CI 1.39-2.00), hospitalization (rate ratio 1.33; 95% CI 1.26-1.40), and all-cause (HR 1.54; 95% CI 1.27-1.86), cardiovascular (HR 2.39; 95% CI 1.69-3.38) and non-cardiovascular (HR 1.27; 95% CI 1.01-1.60) mortality. Additional adjustments for potential mediators (Model 2) showed similar results except that the relations of health literacy with CKD progression and non-cardiovascular mortality were no longer statistically significant.
Conclusions: In the CRIC Study, adults with limited (vs adequate) health literacy had a higher risk for CKD progression, cardiovascular event, hospitalization and mortality-regardless of adjustment for potential confounders.
Keywords: CVD; chronic kidney disease; health literacy; hospitalization; mortality.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
The authors have no financial relationships to disclose. The results presented in this paper have not been published previously in whole or part, except in abstract format.
Figures
References
-
- Institute of Medicine Health literacy: Past, present, and future: Workshop Summary. Washington, DC: The National Academies Press. - PubMed
-
- Gazmararian JA, Williams M V, Peel Jet al. Health literacy and knowledge of chronic disease. Patient Educ Couns 2003;51:267–75. - PubMed
-
- Berkman ND, Sheridan SL, Donahue KEet al. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med 2011;155:97. http://www.ncbi.nlm.nih.gov/pubmed/21768583 - PubMed
Publication types
MeSH terms
Grants and funding
- U54 MD012523/MD/NIMHD NIH HHS/United States
- U01 DK060963/DK/NIDDK NIH HHS/United States
- M01 RR013987/RR/NCRR NIH HHS/United States
- R01 DK119199/DK/NIDDK NIH HHS/United States
- UL1 TR000003/TR/NCATS NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- K01 AG075353/AG/NIA NIH HHS/United States
- U01 DK060990/DK/NIDDK NIH HHS/United States
- UL1 RR029879/RR/NCRR NIH HHS/United States
- U01 DK061028/DK/NIDDK NIH HHS/United States
- UL1 TR000433/TR/NCATS NIH HHS/United States
- K24 DK092290/DK/NIDDK NIH HHS/United States
- R01 DK072231/DK/NIDDK NIH HHS/United States
- U01 DK060984/DK/NIDDK NIH HHS/United States
- U01 DK061021/DK/NIDDK NIH HHS/United States
- U24 DK060990/DK/NIDDK NIH HHS/United States
- U01 DK060980/DK/NIDDK NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- R56 DK072231/DK/NIDDK NIH HHS/United States
- R01 DK118736/DK/NIDDK NIH HHS/United States
- U01 DK061022/DK/NIDDK NIH HHS/United States
- UL1 TR000424/TR/NCATS NIH HHS/United States
- M01 RR016500/RR/NCRR NIH HHS/United States
- P20 GM109036/GM/NIGMS NIH HHS/United States
- U01 DK060902/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
