

Association of obesity with 3-month mortality in kidney failure patients with COVID-19
- PMID: 35747092
- PMCID: PMC8992331
- DOI: 10.1093/ckj/sfac083
Association of obesity with 3-month mortality in kidney failure patients with COVID-19
Abstract
Background: In the general population with coronavirus disease 2019 (COVID-19), obesity is associated with an increased risk of mortality. Given the typically observed obesity paradox among patients on kidney function replacement therapy (KFRT), especially dialysis patients, we examined the association of obesity with mortality among dialysis patients or living with a kidney transplant with COVID-19.
Methods: Data from the European Renal Association COVID-19 Database (ERACODA) were used. KFRT patients diagnosed with COVID-19 between 1 February 2020 and 31 January 2021 were included. The association of Quetelet's body mass index (BMI) (kg/m2), divided into: <18.5 (lean), 18.5-24.9 (normal weight), 25-29.9 (overweight), 30-34.9 (obese I) and ≥35 (obese II/III), with 3-month mortality was investigated using Cox proportional-hazards regression analyses.
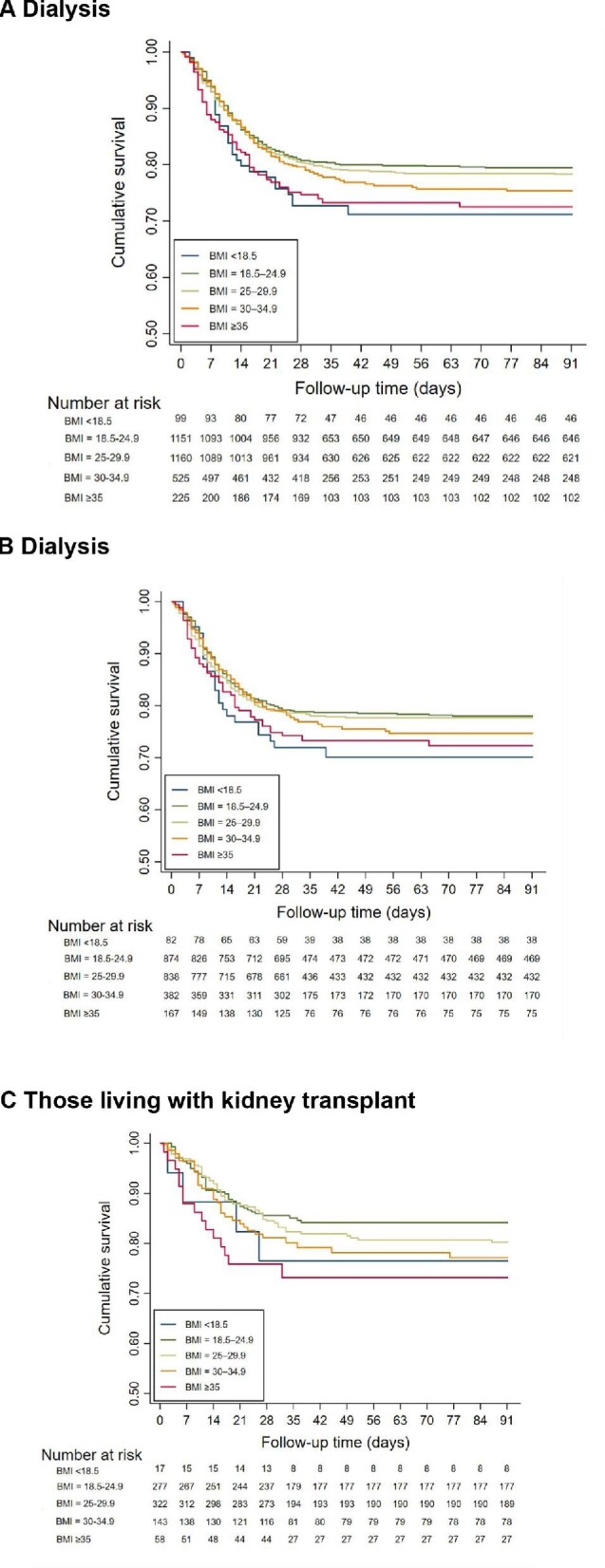
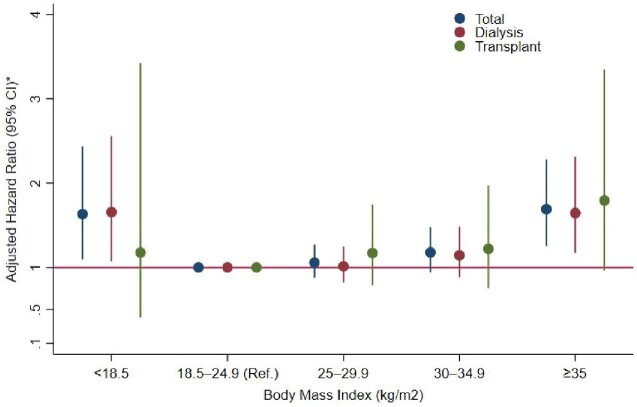
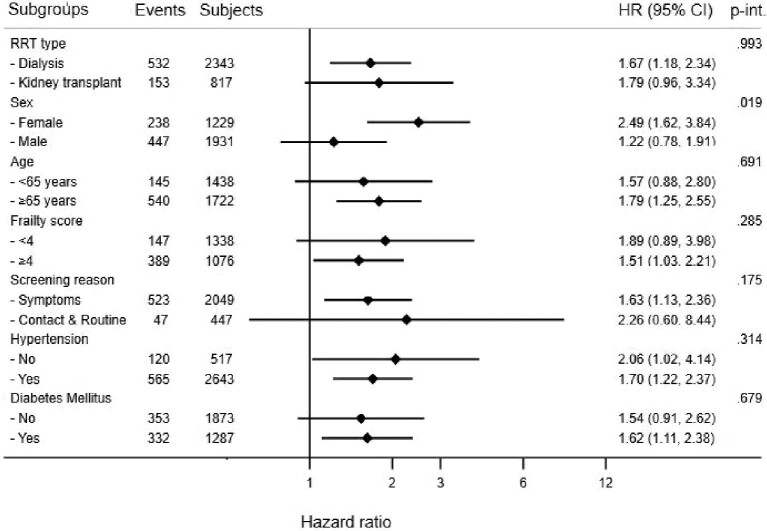
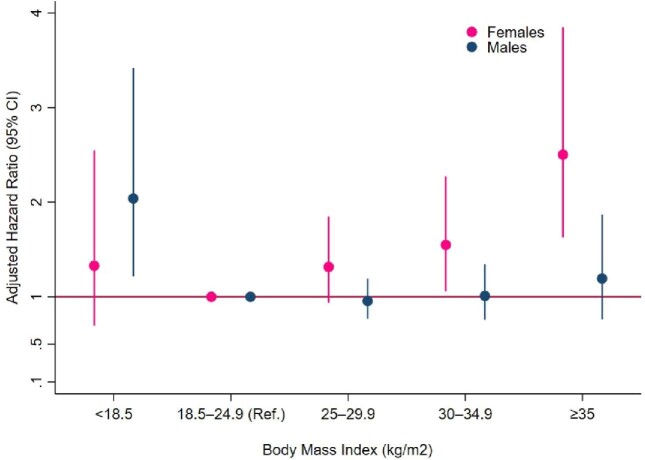
Results: In 3160 patients on KFRT (mean age: 65 years, male: 61%), 99 patients were lean, 1151 normal weight (reference), 1160 overweight, 525 obese I and 225 obese II/III. During follow-up of 3 months, 28, 20, 21, 23 and 27% of patients died in these categories, respectively. In the fully adjusted model, the hazard ratios (HRs) for 3-month mortality were 1.65 [95% confidence interval (CI): 1.10, 2.47], 1 (ref.), 1.07 (95% CI: 0.89, 1.28), 1.17 (95% CI: 0.93, 1.46) and 1.71 (95% CI: 1.27, 2.30), respectively. Results were similar among dialysis patients (N = 2343) and among those living with a kidney transplant (N = 817) (Pinteraction = 0.99), but differed by sex (Pinteraction = 0.019). In males, the HRs for the association of aforementioned BMI categories with 3-month mortality were 2.07 (95% CI: 1.22, 3.52), 1 (ref.), 0.97 (95% CI: 0.78. 1.21), 0.99 (95% CI: 0.74, 1.33) and 1.22 (95% CI: 0.78, 1.91), respectively, and in females corresponding HRs were 1.34 (95% CI: 0.70, 2.57), 1 (ref.), 1.31 (95% CI: 0.94, 1.85), 1.54 (95% CI: 1.05, 2.26) and 2.49 (95% CI: 1.62, 3.84), respectively.
Conclusion: In KFRT patients with COVID-19, on dialysis or a kidney transplant, obesity is associated with an increased risk of mortality at 3 months. This is in contrast to the obesity paradox generally observed in dialysis patients. Additional studies are required to corroborate the sex difference in the association of obesity with mortality.
Keywords: COVID-19; kidney failure; mortality; obesity paradox; reverse epidemiology.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures
References
-
- Kalantar-Zadeh K, Block G, Humphreys MHet al. Reverse epidemiology of cardiovascular risk factors in maintenance dialysis patients. Kidney Int 2003; 63: 793–808 - PubMed
