

Associating factors of suicide and repetition following self-harm: A systematic review and meta-analysis of longitudinal studies
- PMID: 35747199
- PMCID: PMC9126760
- DOI: 10.1016/j.eclinm.2022.101461
Associating factors of suicide and repetition following self-harm: A systematic review and meta-analysis of longitudinal studies
Abstract
Background: Longitudinal evidence for sociodemographic and clinic factors deviating risk for suicide and repetition following SH (self-harm) varied greatly.
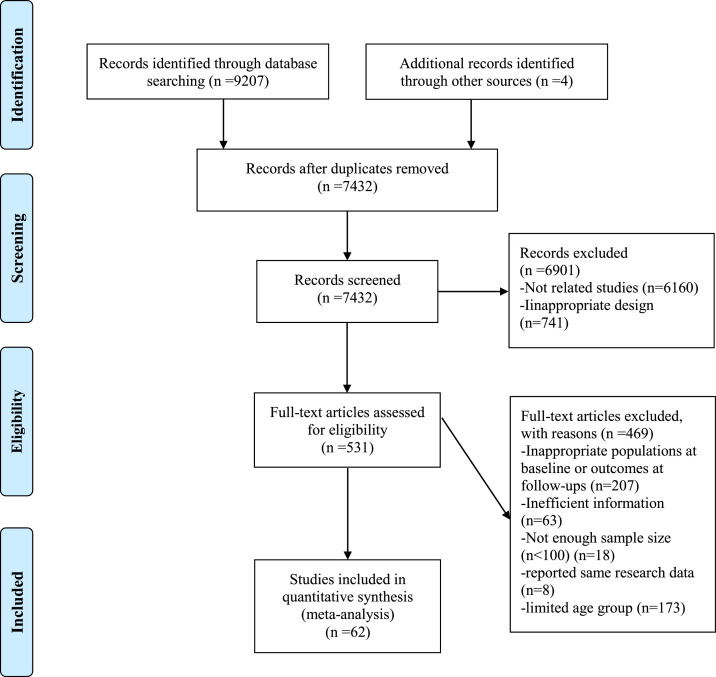
Methods: A comprehensive search of PubMed, Web of Science, EMBASE, and PsycINFO was conducted from January 1st, 2010 to April 5th, 2022. Longitudinal studies focusing on examining associating factors for suicide and repetition following SH were included. PROSPERO registration CRD42021248695.
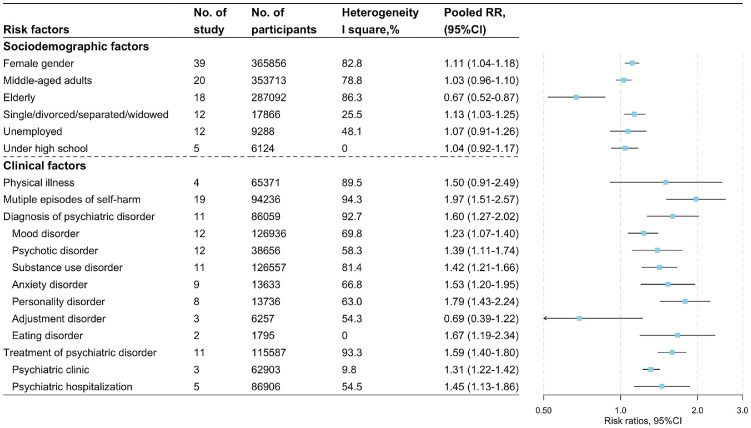
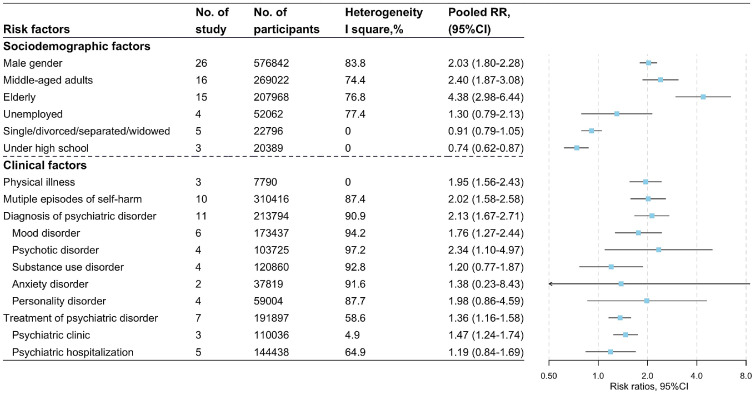
Findings: The present meta-analysis synthesized data from 62 studies published from Jan. 1st, 2010. The associating factors of SH repetition included female gender (RR, 95%CI: 1.11, 1.04-1.18, I2=82.8%), the elderly (compared with adolescents and young adults, RR, 95%CI: 0.67, 0.52-0.87, I2=86.3%), multiple episodes of SH (RR, 95%CI: 1.97, 1.51-2.57, I2=94.3%), diagnosis (RR, 95%CI: 1.60, 1.27-2.02, I2=92.7%) and treatment (RR, 95%CI: 1.59, 1.40-1.80, I2=93.3%) of psychiatric disorder. Male gender (RR, 95%CI: 2.03, 1.80-2.28, I2=83.8%), middle-aged adults (compared with adolescents and young adults, RR, 95%CI: 2.40, 1.87-3.08, I2=74.4%), the elderly (compared with adolescents and young adults, RR, 95%CI: 4.38, 2.98-6.44, I2=76.8%), physical illness (RR, 95%CI: 1.95, 1.56-2.43, I2=0), multiple episodes of SH (RR, 95%CI: 2.02, 1.58-2.58, I2=87.4%), diagnosis (RR, 95%CI: 2.13, 1.67-2.71, I2=90.9%) and treatment (RR, 95%CI: 1.36, 1.16-1.58, I2=58.6%) of psychiatric disorder were associated with increased risk of suicide following SH.
Interpretation: Due to the substantial heterogeneity for clinic factors of suicide and repetition following SH, these results need to be interpreted with caution. Clinics should pay more attention to the cases with SH repetition, especially with poor physical and psychiatric conditions.
Funding: This work was supported by National Natural Science Foundation of China (NSFC) [No: 82103954; 30972527; 81573233].
Keywords: Associating factors; CI, Confidence interval; Meta-analysis; NOS, Newcastle-Ottawa Scale; RR, Risk ratio; Repetition; SA, Suicide attempt; SC, Self-cutting; SH, Self-harm; SP, Self-poisoning; Self-harm; Suicide.
© 2022 The Author(s).
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Hawton K., Zahl D., Weatherall R. Suicide following deliberate self-harm: long-term follow-up of patients who presented to a general hospital. Br J Psychiatry. 2003;182:537–542. - PubMed
-
- GBD 2015 DALYs and HALE Collaborators Global, regional, and national disability-adjusted life-years (DALYs) for 315 diseases and injuries and healthy life expectancy (HALE), 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1603–1658. - PMC - PubMed
-
- World Health Organization. Practice Manual For Establishing and Maintaining Surveillance Systems For Suicide Attempts and Self-Harm. 2016. https://www.who.int/mental_health/suicide-prevention/attempts_surveillan....
LinkOut - more resources
Full Text Sources
Miscellaneous
