

Epidemiology, Healthcare Resource Utilization, and Mortality of Asthma and COPD in COVID-19: A Systematic Literature Review and Meta-Analyses
- PMID: 35747745
- PMCID: PMC9211747
- DOI: 10.2147/JAA.S360985
Epidemiology, Healthcare Resource Utilization, and Mortality of Asthma and COPD in COVID-19: A Systematic Literature Review and Meta-Analyses
Abstract
Purpose: There has been concern that asthma and chronic obstructive pulmonary disease [COPD] increase the risk of developing and exacerbating COVID-19. The effect of medications such as inhaled corticosteroids (ICS) and biologics on COVID-19 is unclear. This systematic literature review analyzed the published evidence on epidemiology and the burden of illness of asthma and COPD, and the use of baseline medicines among COVID-19 populations.
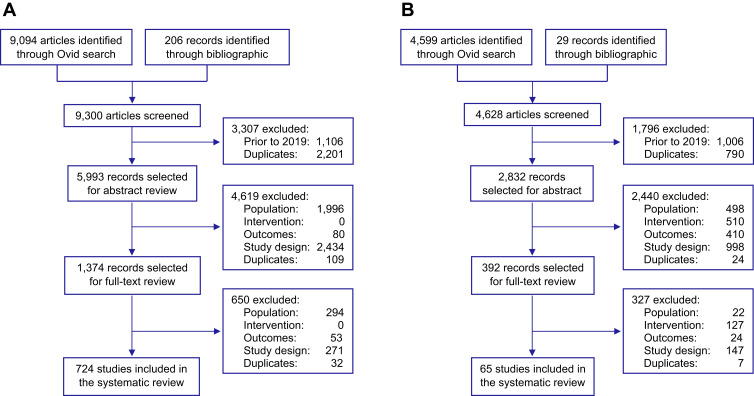
Patients and methods: Using Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, Embase®, MEDLINE® and Cochrane were searched (January 2019-August 2021). The prevalence of asthma or COPD among COVID-19 populations was compared to the country-specific populations. Odds ratios (ORs) were estimated to compare healthcare resource utilization (HCRU) rates, and meta-analyses of outcomes were estimated from age-adjusted ORs (aORs) or hazard ratios (aHRs). Meta-analyses of COVID-19 outcomes were conducted using random effects models for binary outcomes.
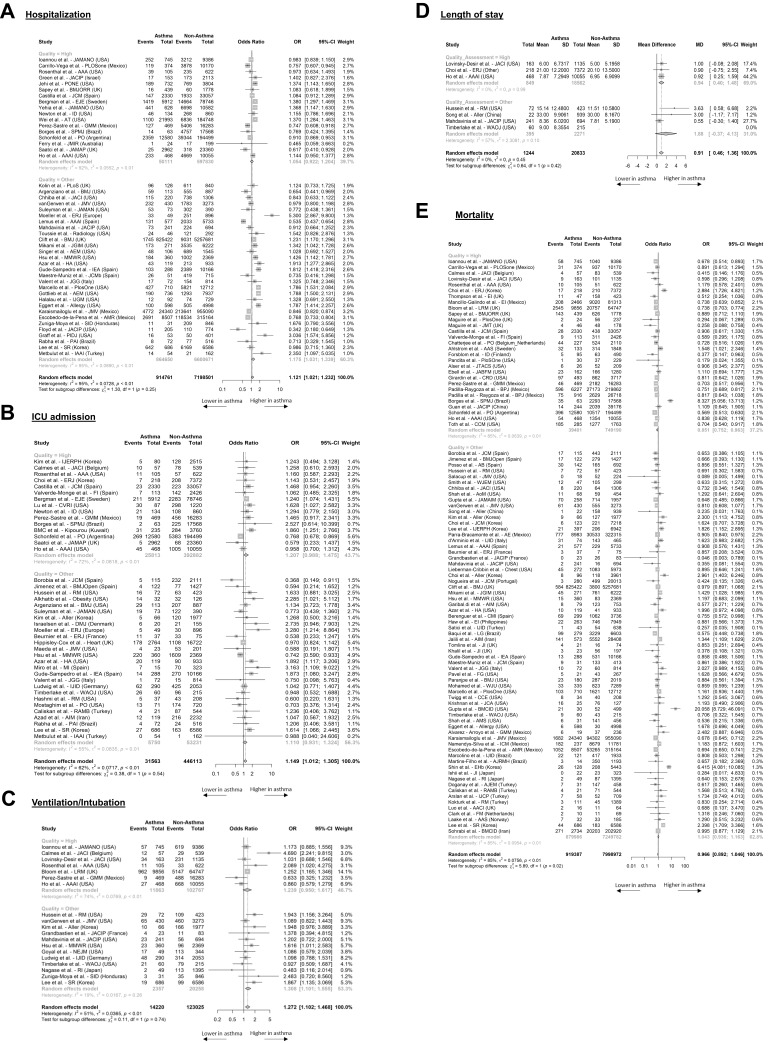
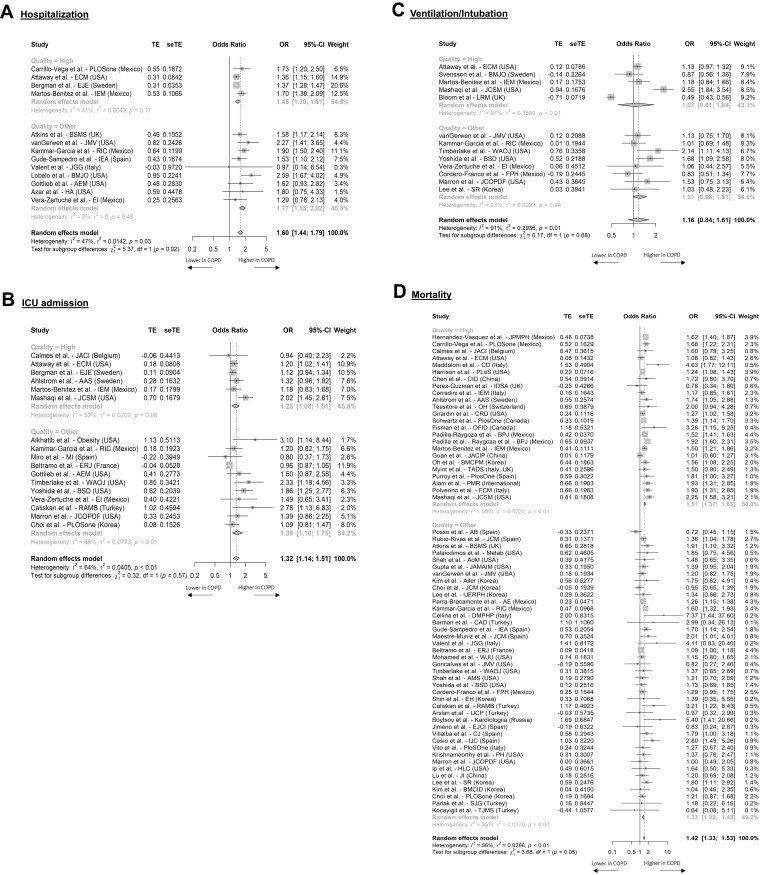
Results: Given the number and heterogeneity of studies, only 183 high-quality studies were analyzed, which reported hospitalization, intensive care unit (ICU) admissions, ventilation/intubation, or mortality. Asthma patients were not at increased risk for COVID-19-related hospitalization (OR = 1.05, 95% CI: 0.92 to 1.20), ICU admission (OR = 1.21, 95% CI: 0.99 to 1.1.48), ventilation/intubation (OR = 1.24, 95% CI: 0.95 to 1.62), or mortality (OR = 0.85, 95% CI: 0.75 to 0.96). Accounting for confounding variables, COPD patients were at higher risk of hospitalization (aOR = 1.45, 95% CI: 1.30 to 1.61), ICU admission (aOR = 1.28, 95% CI: 1.08 to 1.51), and mortality (aOR = 1.41, 95% CI: 1.37 to 1.65). Sixty-five studies reported outcomes associated with ICS or biologic use. There was limited evidence that ICS or biologics significantly impacted the risk of SARS-CoV-2 infection, HCRU, or mortality in asthma or COPD patients.
Conclusion: In high-quality studies included, patients with asthma were not at significantly higher odds for adverse COVID-19-related outcomes, while patients with COPD were at higher odds. There was no clear evidence that baseline medication affected outcomes.
Registration: PROSPERO (CRD42021233963).
Keywords: SARS-COV-2; biologics; healthcare resource utilization; inhaled corticosteroids; mortality.
© 2022 Halpin et al.
Conflict of interest statement
This study was funded by AstraZeneca (AZ) and Way’s Group. The following AZ and Way’s Group employees were involved in the study design, decision to publish, and preparation of the manuscript: Professor Adrian Rabe and Dr. Wei Jie Loke. Professor Adrian Rabe reports grants from AstraZeneca, during the conduct of the study. Dr. Wei Jie Loke reports personal fees from AstraZeneca UK, during the conduct of the study. Professor David Halpin was an external consultant. Professor David Halpin reports personal fees from Aerogen, AstraZeneca, Boehringer Ingelheim, Chiesi, CSL Behring, GSK, Novartis, Pfizer, Sanofi, outside the submitted work. Stacy Grieve, Patrick Daniele, Sanghee Hwang, and Anna Forsythe are employees of Purple Squirrel Economics, a Cytel Company, which was a paid consultant to AstraZeneca in connection with the development of this manuscript. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
The Risk of COVID-19 Related Hospitalsation, Intensive Care Unit Admission and Mortality in People With Underlying Asthma or COPD: A Systematic Review and Meta-Analysis.Front Med (Lausanne). 2021 Jun 16;8:668808. doi: 10.3389/fmed.2021.668808. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34222281 Free PMC article.
-
Outcomes of COVID-19 amongst patients with ongoing use of inhaled corticosteroids - a systematic review & meta-analysis.Infez Med. 2023 Dec 1;31(4):440-448. doi: 10.53854/liim-3104-3. eCollection 2023. Infez Med. 2023. PMID: 38075428 Free PMC article. Review.
-
The influence of prior use of inhaled corticosteroids on COVID-19 outcomes: A systematic review and meta-analysis.PLoS One. 2024 Jan 19;19(1):e0295366. doi: 10.1371/journal.pone.0295366. eCollection 2024. PLoS One. 2024. PMID: 38241229 Free PMC article.
-
Regular Inhaled Corticosteroids Use May Protect Against Severe COVID-19 Outcome in COPD.Int J Chron Obstruct Pulmon Dis. 2023 Aug 7;18:1701-1712. doi: 10.2147/COPD.S404913. eCollection 2023. Int J Chron Obstruct Pulmon Dis. 2023. PMID: 37576828 Free PMC article.
-
Risks of infection, hospital and ICU admission, and death from COVID-19 in people with asthma: systematic review and meta-analyses.BMJ Evid Based Med. 2022 Oct;27(5):263-273. doi: 10.1136/bmjebm-2021-111788. Epub 2021 Dec 21. BMJ Evid Based Med. 2022. PMID: 34933924
Cited by
-
Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2023 Guidelines Reviewed.Open Respir Med J. 2024 Jan 10;18:e18743064279064. doi: 10.2174/0118743064279064231227070344. eCollection 2024. Open Respir Med J. 2024. PMID: 38660684 Free PMC article. Review.
-
Clinical and laboratory factors associated with mortality among hospitalized patients with COVID-19 infection in Lebanon: A multicenter study.PLoS One. 2022 Dec 1;17(12):e0278393. doi: 10.1371/journal.pone.0278393. eCollection 2022. PLoS One. 2022. PMID: 36454777 Free PMC article.
-
Impact of SARS-CoV-2 infective exacerbation of chronic obstructive pulmonary disease on clinical outcomes in a prospective cohort study of hospitalised adults.J R Soc Med. 2023 Nov;116(11):371-385. doi: 10.1177/01410768231184162. Epub 2023 Jul 5. J R Soc Med. 2023. PMID: 37404021 Free PMC article.
-
Impact and prevalence of comorbidities and complications on the severity of COVID-19 in association with age, gender, obesity, and pre-existing smoking: A meta-analysis.Biomedicine (Taipei). 2024 Mar 1;14(1):20-38. doi: 10.37796/2211-8039.1429. eCollection 2024. Biomedicine (Taipei). 2024. PMID: 38533301 Free PMC article. Review.
-
Global burden of major chronic respiratory diseases among older adults aged 55 and above from 1990 to 2021: Changes, challenges, and predictions amid the pandemic.PLoS One. 2025 Aug 1;20(8):e0329283. doi: 10.1371/journal.pone.0329283. eCollection 2025. PLoS One. 2025. PMID: 40749041 Free PMC article.
References
-
- Global surveillance, prevention and control of chronic respiratory diseases. Available from: https://www.who.int/publications-detail-redirect/global-surveillance-pre.... Accessed March 26, 2021.
-
- CDC. COVID-19 and your health. Centers for disease control and prevention; 2020. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-.... Accessed March 19, 2021.
LinkOut - more resources
Full Text Sources
Miscellaneous
