

What Affects Segmental Lordosis of the Surgical Site after Minimally Invasive Transforaminal Lumbar Interbody Fusion?
- PMID: 35748078
- PMCID: PMC9226838
- DOI: 10.3349/ymj.2022.63.7.665
What Affects Segmental Lordosis of the Surgical Site after Minimally Invasive Transforaminal Lumbar Interbody Fusion?
Abstract
Purpose: This study was undertaken to identify factors that affect segmental lordosis (SL) after minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) by comparing patients whose postoperative SL increased with those whose decreased.
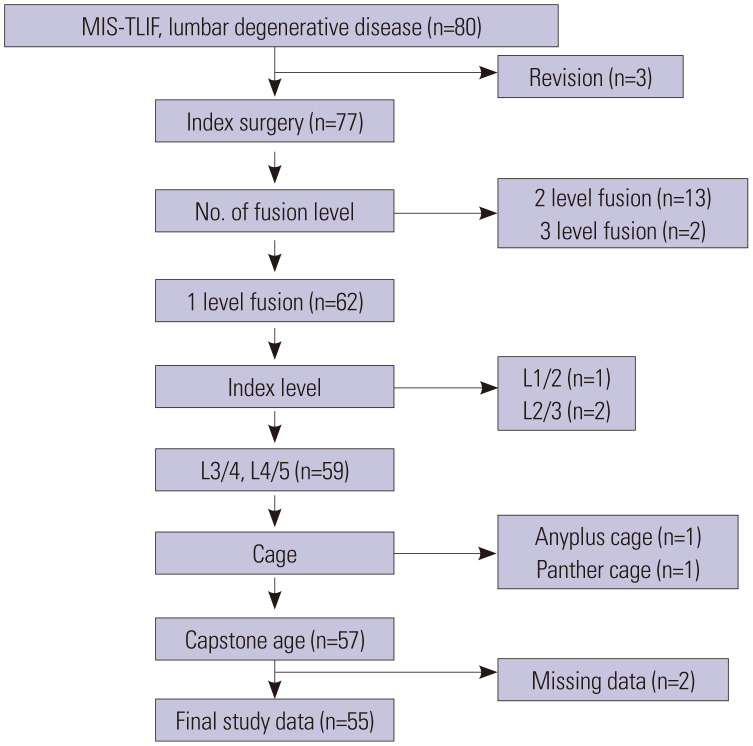
Materials and methods: Fifty-five patients underwent MIS-TLIF at our institute from January 2018 to September 2019. Demographic, pre- and postoperative radiologic, and cage-related factors were included. Statistical analyses were designed to compare patients whose SL increased with decreased after surgery.
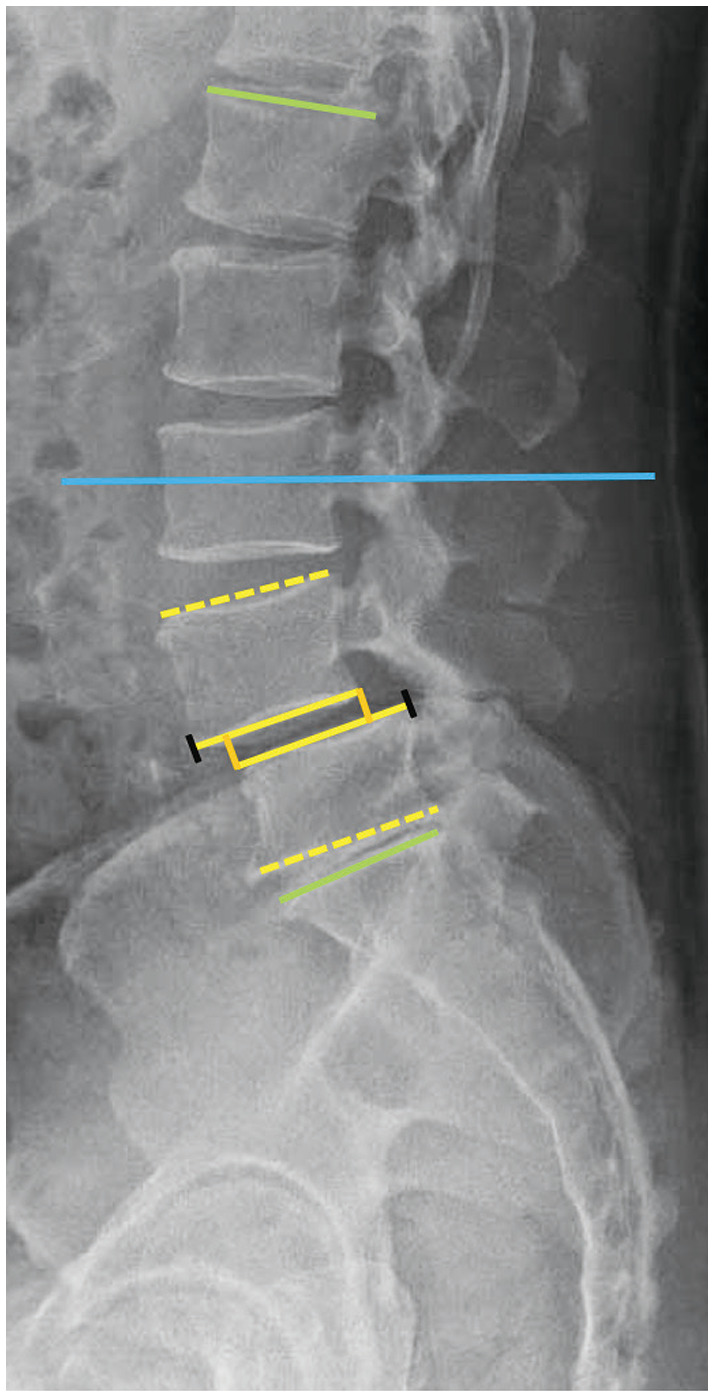
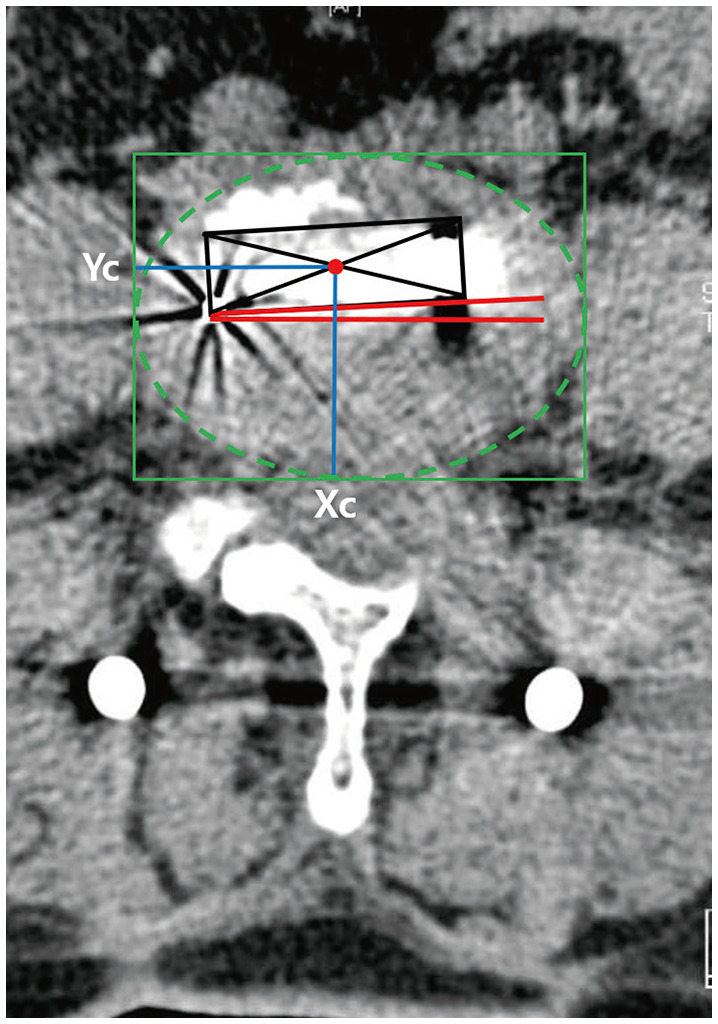
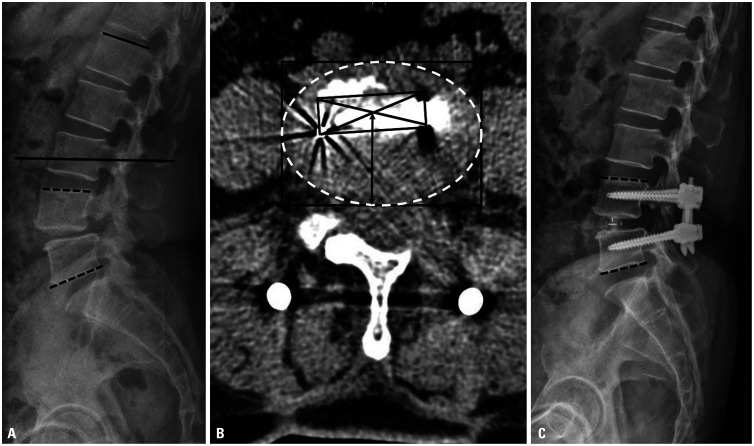
Results: After surgery, SL increased in 34 patients (group I) and decreased in 21 patients (group D). The index level, disc lordosis, SL, lumbar lordosis, proximal lordosis (PL), and Y-axis position of the cage (Yc) differed significantly between groups I and D. The cage in group I was more anterior than that in group D (Yc: 55.84% vs. 51.24%). Multivariate analysis showed that SL decreased more significantly after MIS-TLIF when the index level was L3/4 rather than L4/5 [odds ratio (OR): 0.46, p=0.019], as preoperative SL (OR: 0.82, p=0.037) or PL (OR: 0.68, p=0.028) increased, and as the cage became more posterior (OR: 1.10, p=0.032).
Conclusion: Changes in SL after MIS-TLIF appear to be associated with preoperative SL and PL, index level, and Yc. An index level at L4/5 instead of L3/4, smaller preoperative SL or PL, and an anterior position of the cage are likely to result in increased SL after MIS-TLIF.
Keywords: Minimally invasive; cage; lumbar lordosis; outcome; segmental lordosis; spine surgery; transforaminal lumbar interbody fusion.
© Copyright: Yonsei University College of Medicine 2022.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Tian H, Wu A, Guo M, Zhang K, Chen C, Li X, et al. Adequate restoration of disc height and segmental lordosis by lumbar interbody fusion decreases adjacent segment degeneration. World Neurosurg. 2018;118:e856–e864. - PubMed
-
- Brodano GB, Martikos K, Lolli F, Gasbarrini A, Cioni A, Bandiera S, et al. Transforaminal lumbar interbody fusion in degenerative disk disease and spondylolisthesis grade I: minimally invasive versus open surgery. J Spinal Disord Tech. 2015;28:E559–E564. - PubMed
-
- Lee WC, Park JY, Kim KH, Kuh SU, Chin DK, Kim KS, et al. Minimally invasive transforaminal lumbar interbody fusion in multilevel: comparison with conventional transforaminal interbody fusion. World Neurosurg. 2016;85:236–243. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
