

Contemporary Unplanned Readmission Trends Following Management of Type B Aortic Dissection
- PMID: 35748179
- PMCID: PMC9233985
- DOI: 10.5758/vsi.220007
Contemporary Unplanned Readmission Trends Following Management of Type B Aortic Dissection
Abstract
Purpose: Large studies have demonstrated improved survival outcomes with thoracic endovascular aortic repair (TEVAR) at two and five years compared to medical therapy; however, early TEVAR for acute type B aortic dissection (TBAD) remains controversial. We aimed to evaluate trends and clinical predictors of hospital readmissions in patients undergoing medical management and TEVAR for acute TBADs.
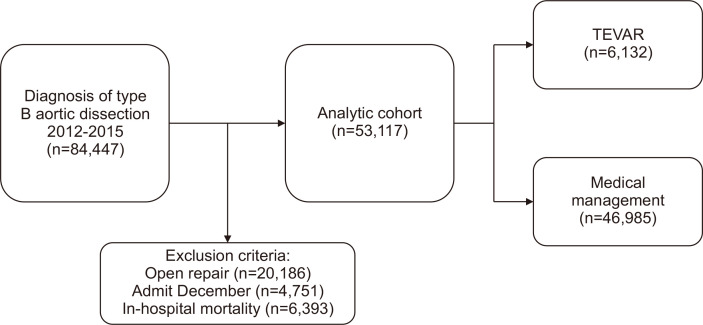
Materials and methods: The Nationwide Readmissions Database was queried for all 30-day and 90-day index readmissions (30D-IR and 90D-IR, respectively) after a diagnosis of a TBAD from January 2012 to September 2015. Data on readmission diagnosis, patient demographics, and hospital characteristics were collected from readmitted patients and analyzed. Multivariable logistic regression models were used to identify the predictors of readmission after TEVAR or medical medical management of TBAD.
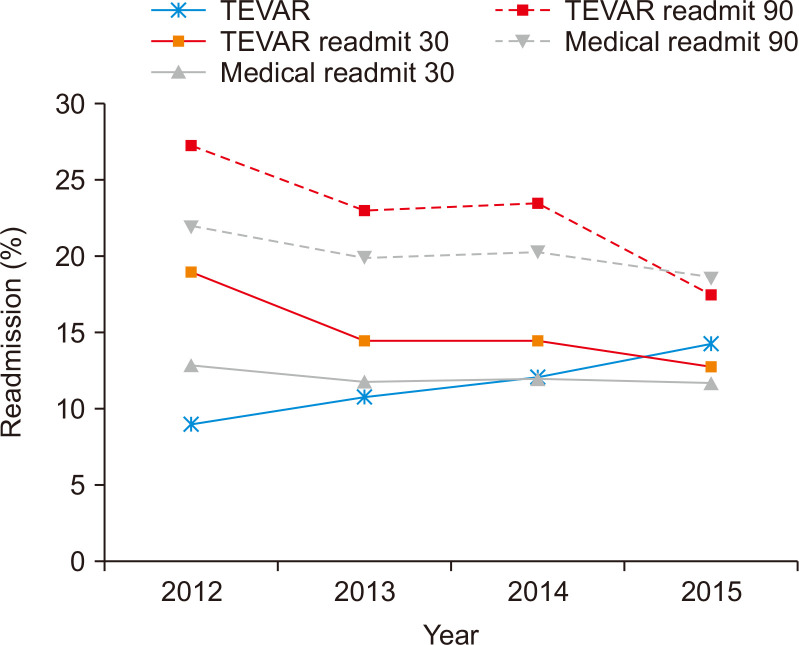
Results: We identified 53,117 patients with acute TBAD. Medical management was the initial treatment modality in 46,985 (88.4%) patients, while 6,132 (11.5%) underwent TEVAR. Factors including older patient age, lower household income, severity of comorbidities, initial hospital length of stay, and urgent procedure demonstrated an increased likelihood of experiencing 30D-IR and 90D-IR (P<0.05). The rate of unplanned readmission for patients undergoing medical management remained stable (11.3% vs. 10.0% for 30D-IR; 19.1% vs. 15.5% for 90D-IR). Reasons for unplanned readmission in the TEVAR cohort were largely related to technical complications. There was no significant difference in readmission costs between medical management and TEVAR.
Conclusion: Number of unplanned readmissions in the TEVAR arm decreased significantly over time, whereas the number of readmissions for medical management remained stable.
Keywords: Aortic dissection; Nationwide readmissions database; Readmission; Thoracic endovascular aortic repair; Type B dissection.
Conflict of interest statement
The authors have nothing to disclose.
Figures
References
-
- Nienaber CA, Kische S, Rousseau H, Eggebrecht H, Rehders TC, Kundt G, et al. Endovascular repair of type B aortic dissection: long-term results of the randomized investigation of stent grafts in aortic dissection trial. Circ Cardiovasc Interv. 2013;6:407–416. doi: 10.1161/CIRCINTERVENTIONS.113.000463. - DOI - PubMed
LinkOut - more resources
Full Text Sources
