

Effect of Automated Telephone Infectious Disease Consultations to Nonacademic Hospitals on 30-Day Mortality Among Patients With Staphylococcus aureus Bacteremia: The SUPPORT Cluster Randomized Clinical Trial
- PMID: 35749114
- PMCID: PMC9233240
- DOI: 10.1001/jamanetworkopen.2022.18515
Effect of Automated Telephone Infectious Disease Consultations to Nonacademic Hospitals on 30-Day Mortality Among Patients With Staphylococcus aureus Bacteremia: The SUPPORT Cluster Randomized Clinical Trial
Abstract
Importance: Staphylococcus aureus bacteremia (SAB) is a common and potentially severe infectious disease (ID). Retrospective studies and derived meta-analyses suggest that bedside infectious disease consultation (IDC) for SAB is associated with improved survival; however, such IDCs might not always be possible because of the lack of ID specialists, particularly at nonacademic hospitals.
Objectives: To investigate whether unsolicited telephone IDCs (triggered by an automated blood stream infection reporting system) to nonacademic hospitals improved 30-day all-cause mortality in patients with SAB.
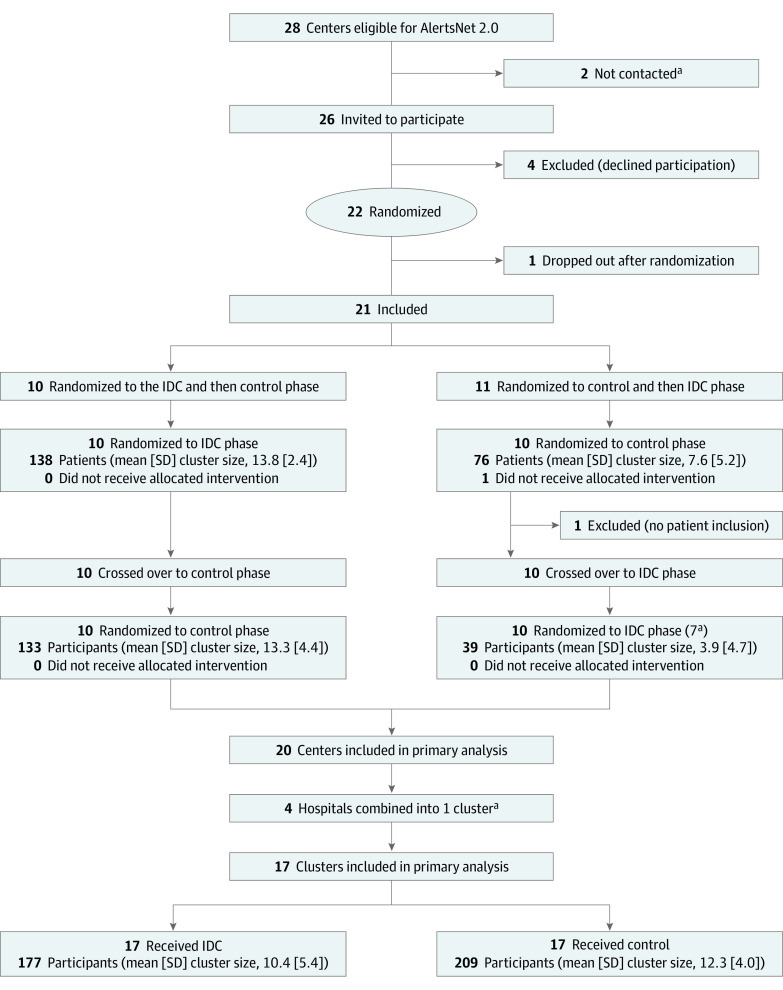
Design, setting, and participants: This patient-blinded, multicenter, interventional, cluster randomized, controlled, crossover clinical trial was conducted in 21 rural, nonacademic hospitals in Thuringia, Germany. From July 1, 2016, to December 31, 2018, 1029 blood culture reports were assessed for eligibility. A total of 386 patients were enrolled, whereas 643 patients were not enrolled for the following reasons: death before enrollment (n = 59); palliative care (n = 41); recurrence of SAB (n = 9); discharge from the hospital before enrollment (n = 77); age younger than 18 years (n = 5); duplicate report from a single patient (n = 26); late report (n = 17); blood culture reported during the washout phase (n = 48); and no signed informed consent for other or unknown reasons (n = 361).
Interventions: During the ID intervention phase, ID specialists from Jena University Hospital provided unsolicited telephone IDCs to physicians treating patients with SAB. During the control phase, patients were treated according to local standards. Crossover was performed after including 15 patients or, at the latest, 1 year after the first patient was included.
Main outcomes and measures: Thirty-day all-cause mortality.
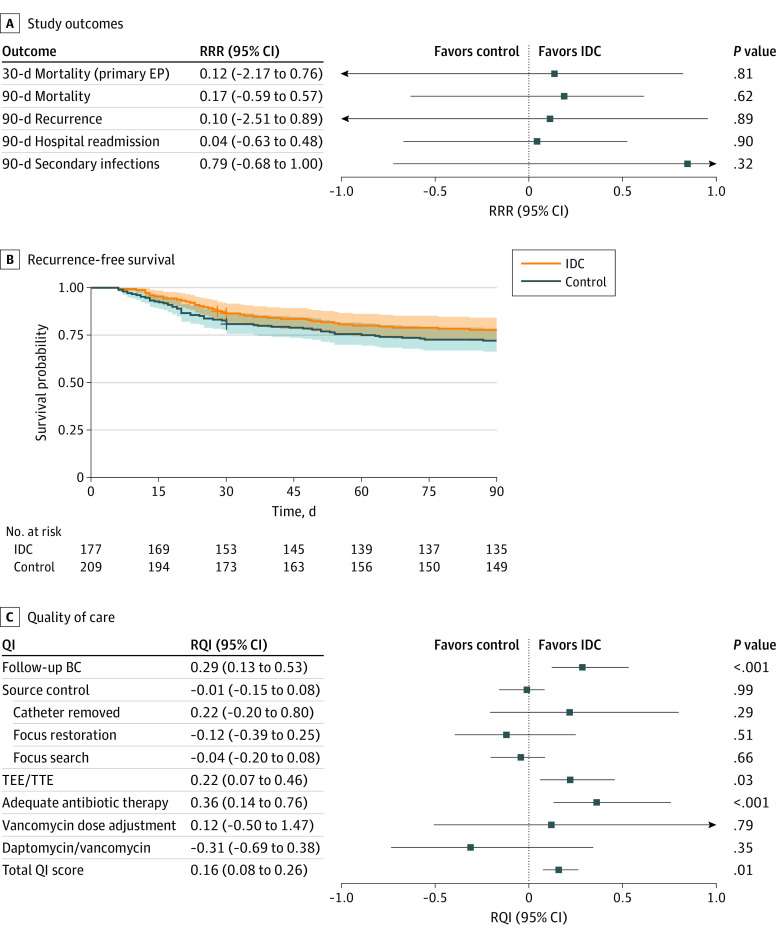
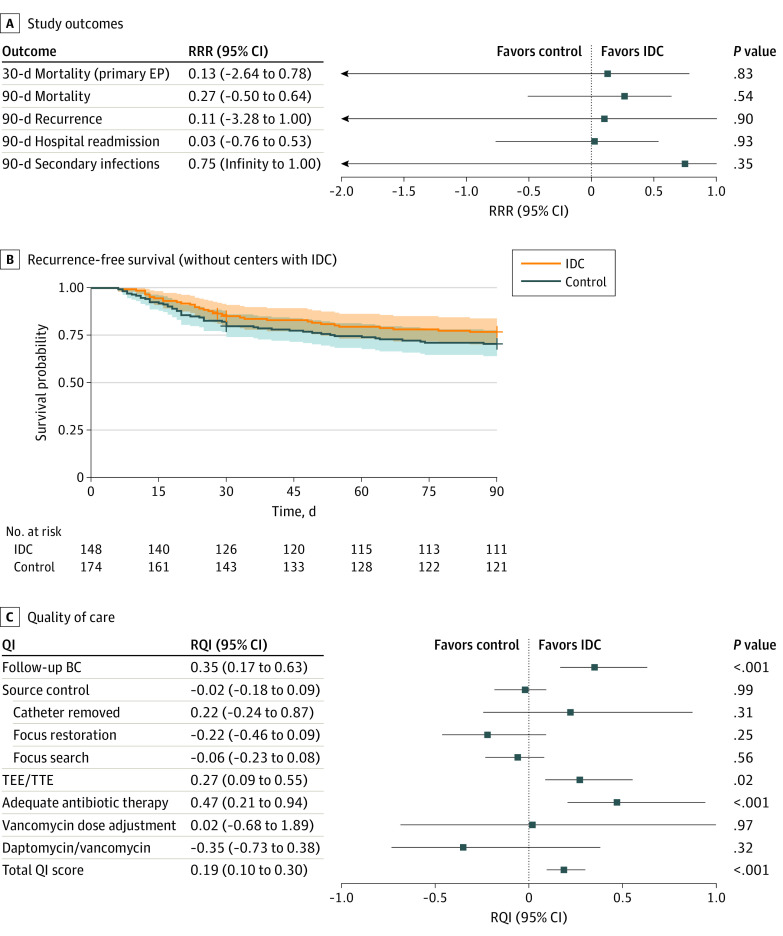
Results: A total of 386 patients (median [IQR] age, 75 [63-82] years; 261 [67.6%] male) were included, with 177 randomized to the IDC group and 209 to the control group. The 30-day all-cause mortality rate did not differ between the IDC and control groups (relative risk reduction [RRR], 0.12; 95% CI, -2.17 to 0.76; P = .81). No evidence was found of a difference in secondary outcomes, including 90-day mortality (RRR, 0.17; 95% CI, -0.59 to 0.57; P = .62), 90-day recurrence (RRR, 0.10; 95% CI, -2.51 to 0.89; P = .89), and hospital readmission (RRR, 0.04; 95% CI, -0.63 to 0.48; P = .90). Exploratory evidence suggested that indicators of quality of care were potentially realized more often in the IDC group than in the control group (relative quality improvement, 0.16; 95% CI, 0.08-0.26; P = .01).
Conclusions and relevance: In this cluster randomized clinical trial, unsolicited telephone IDC, although potentially enhancing quality of care, did not improve 30-day all-cause mortality in patients with SAB.
Trial registration: drks.de Identifier: DRKS00010135.
Conflict of interest statement
Figures
References
-
- Madaline T, Wadskier Montagne F, Eisenberg R, et al. . Early infectious disease consultation is associated with lower mortality in patients with severe sepsis or septic shock who complete the 3-hour sepsis treatment bundle. Open Forum Infect Dis. 2019;6(10):ofz408. doi:10.1093/ofid/ofz408 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
