

Targeting signaling pathways in prostate cancer: mechanisms and clinical trials
- PMID: 35750683
- PMCID: PMC9232569
- DOI: 10.1038/s41392-022-01042-7
Targeting signaling pathways in prostate cancer: mechanisms and clinical trials
Abstract
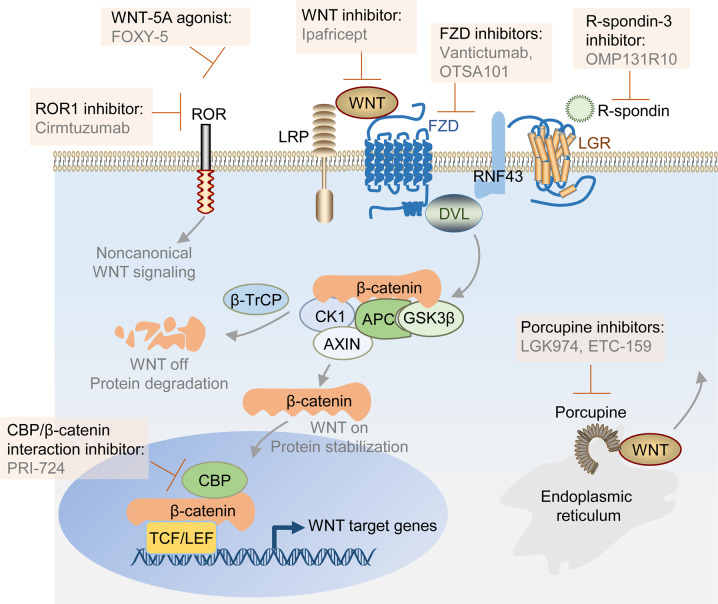
Prostate cancer (PCa) affects millions of men globally. Due to advances in understanding genomic landscapes and biological functions, the treatment of PCa continues to improve. Recently, various new classes of agents, which include next-generation androgen receptor (AR) signaling inhibitors (abiraterone, enzalutamide, apalutamide, and darolutamide), bone-targeting agents (radium-223 chloride, zoledronic acid), and poly(ADP-ribose) polymerase (PARP) inhibitors (olaparib, rucaparib, and talazoparib) have been developed to treat PCa. Agents targeting other signaling pathways, including cyclin-dependent kinase (CDK)4/6, Ak strain transforming (AKT), wingless-type protein (WNT), and epigenetic marks, have successively entered clinical trials. Furthermore, prostate-specific membrane antigen (PSMA) targeting agents such as 177Lu-PSMA-617 are promising theranostics that could improve both diagnostic accuracy and therapeutic efficacy. Advanced clinical studies with immune checkpoint inhibitors (ICIs) have shown limited benefits in PCa, whereas subgroups of PCa with mismatch repair (MMR) or CDK12 inactivation may benefit from ICIs treatment. In this review, we summarized the targeted agents of PCa in clinical trials and their underlying mechanisms, and further discussed their limitations and future directions.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures






References
-
- Disease GBD, Injury I, Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. doi: 10.1016/S0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- Foreman KJ, et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet. 2018;392:2052–2090. doi: 10.1016/S0140-6736(18)31694-5. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
