

Transcranial magnetic stimulation in the treatment of adolescent depression: a systematic review and meta-analysis of aggregated and individual-patient data from uncontrolled studies
- PMID: 35751003
- PMCID: PMC9532325
- DOI: 10.1007/s00787-022-02021-7
Transcranial magnetic stimulation in the treatment of adolescent depression: a systematic review and meta-analysis of aggregated and individual-patient data from uncontrolled studies
Abstract
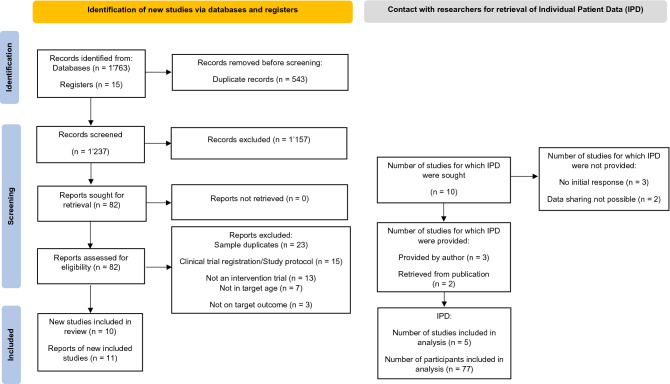
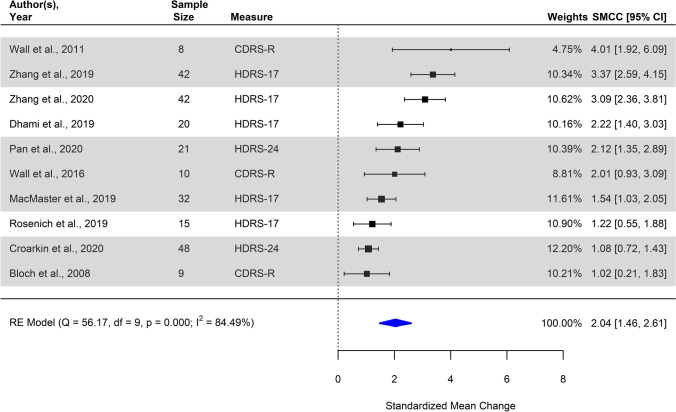
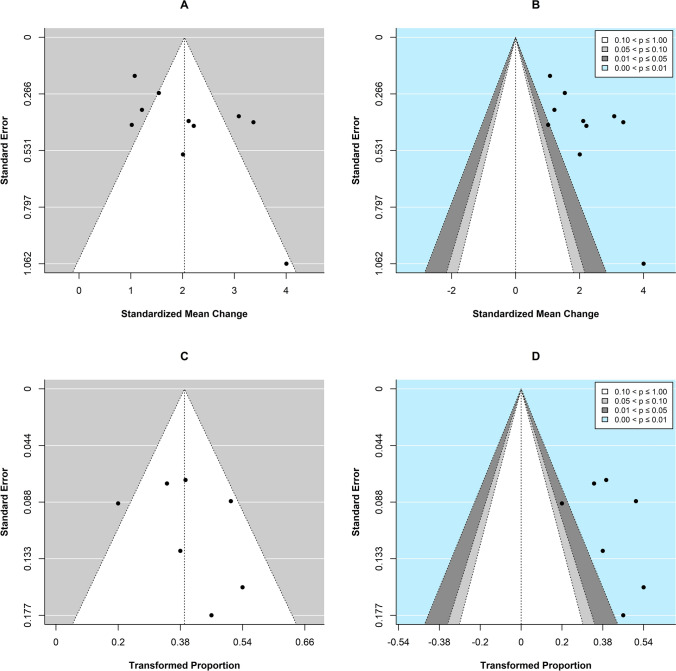
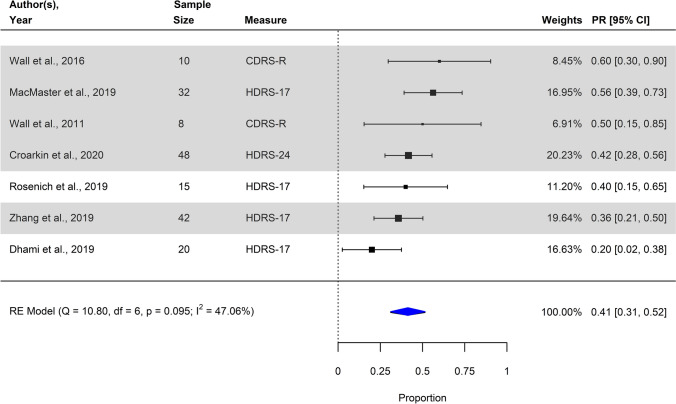
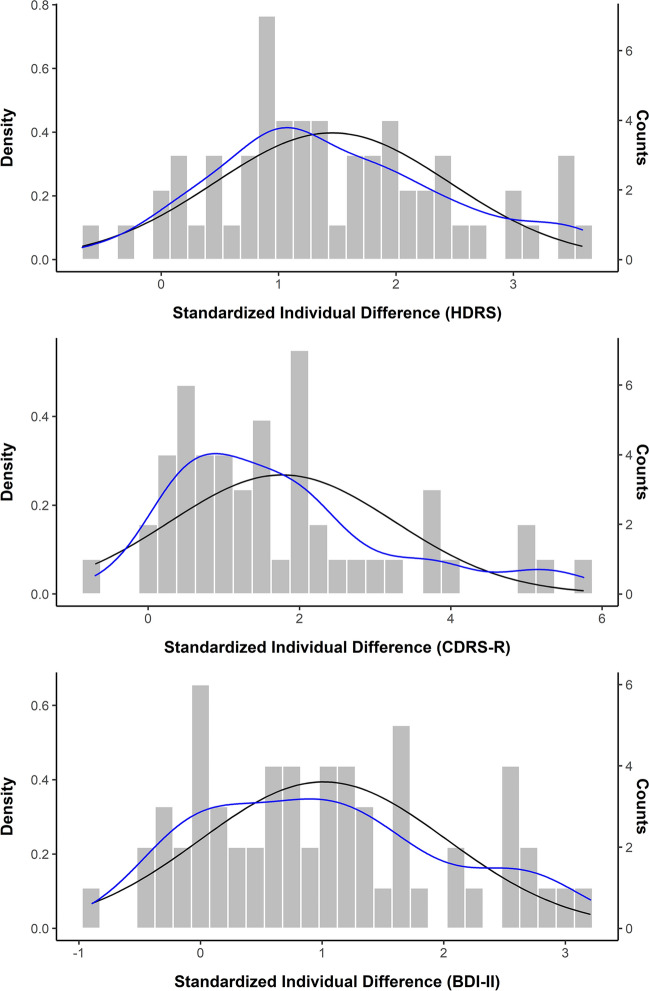
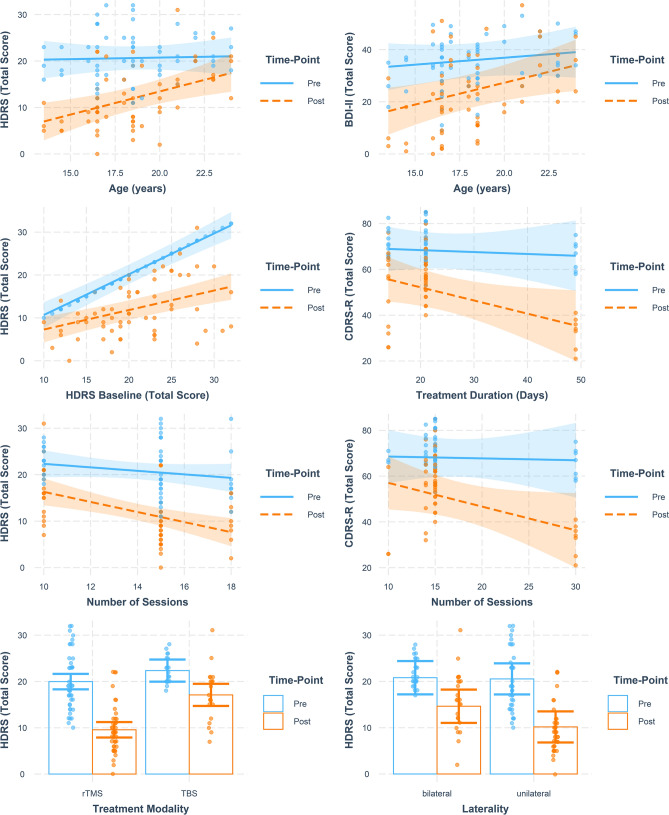
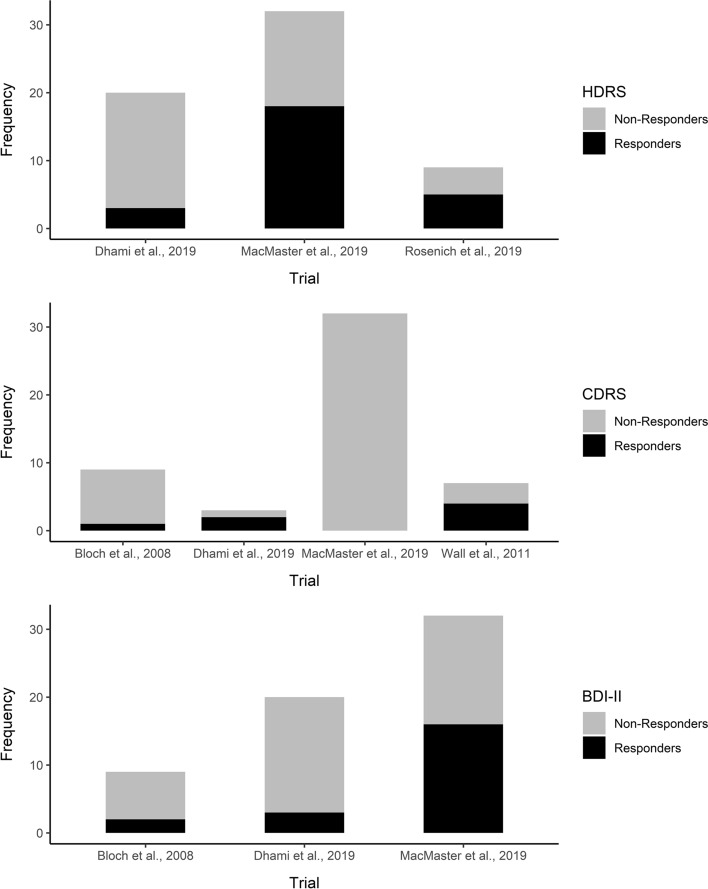
Transcranial magnetic stimulation (TMS) is a non-invasive treatment for adolescent major depressive disorder (MDD). Existing evidence on the efficacy of TMS in adolescent MDD awaits quantitative synthesis. A systematic literature search was conducted, and data from eligible studies were synthesized using random-effects models. Treatment-covariate interactions were examined in exploratory analyses of individual-patient data (IPD). Systematic search of the literature yielded 1264 hits, of which 10 individual studies (2 randomized trials) were included for quantitative synthesis of mainly uncontrolled studies. Individual patient data (IPD) were available from five trials (all uncontrolled studies). Quantitative synthesis of aggregated data revealed a statistically significant negative overall standardized mean change (pooled SMCC = 2.04, 95% CI [1.46; 2.61], SE = 0.29, p < .001), as well as a significant overall treatment response rate (Transformed Proportion = 41.30%, 95% CI [31.03; 51.57], SE = 0.05; p < 0.001), considering data from baseline to post-treatment. Exploratory IPD analyses suggests TMS might be more effective in younger individuals and individuals with more severe depression, and efficacy might be enhanced with certain treatment modality settings, including higher number of TMS sessions, longer treatment durations, and unilateral and not bilateral stimulation. Existing studies exhibit methodological shortcomings, including small-study effects and lack of control group, blinding, and randomization-compromising the credibility of the present results. To date, two randomized controlled trials on TMS in adolescent depression have been published, and the only large-scale randomized trial suggests TMS is not more effective than sham stimulation. Future large-scale, randomized, and sham-controlled trials are warranted. Future trials should ensure appropriate selection of patients for TMS treatment and guide precision medicine approaches for stimulation protocols.
Keywords: Adolescence; Individual patient data; Major depressive disorder; Meta-analysis; Transcranial magnetic stimulation.
© 2022. The Author(s).
Conflict of interest statement
Dr. Croarkin is supported by National Institute of Mental Health awards R01MH113700 and R01MH124655. The content is solely the responsibility of the authors and does not necessarily reflect the official views of the National Institute of Mental Health or the National Institutes of Health. Dr. MacMaster is supported by the Alberta Children’s Hospital Foundation and the Canadian Institute of Health Research.
Figures
Comment in
-
Connectome-guided transcranial magnetic stimulation treatment in depression.Eur Child Adolesc Psychiatry. 2022 Oct;31(10):1481-1483. doi: 10.1007/s00787-022-02089-1. Eur Child Adolesc Psychiatry. 2022. PMID: 36151354 No abstract available.
References
-
- Zhou X, et al. Comparative efficacy and acceptability of antidepressants, psychotherapies, and their combination for acute treatment of children and adolescents with depressive disorder: a systematic review and network meta-analysis. Lancet Psychiatry. 2020;7(7):581–601. doi: 10.1016/S2215-0366(20)30137-1. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
