

Molecular epidemiological surveillance of viral agents of acute lower respiratory tract infections in children in Accra, Ghana
- PMID: 35751110
- PMCID: PMC9229459
- DOI: 10.1186/s12887-022-03419-7
Molecular epidemiological surveillance of viral agents of acute lower respiratory tract infections in children in Accra, Ghana
Abstract
Background: Acute lower respiratory tract infection (ALRTI) in children under 5 years is known to be predominantly caused by respiratory syncytial virus (RSV). In recent times, however, human metapneumovirus (HMPV) has also been implicated. This study sought to investigate and genotype respiratory syncytial virus and human metapneumovirus in children presenting with ALRTIs infection at the Princess Marie Louis Children's Hospital in Accra, Ghana.
Methods: Children below 5 years who were clinically diagnosed of ALRTI and on admission at the study site were recruited between September 2015 and November 2016 for this study. Demographic data information was obtained by means of a standardized questionnaire; and relevant clinical information was obtained from medical records. Nasopharyngeal swabs were collected from 176 children recruited for the study. Ribonucleic acid was extracted from swabs and cDNA syntheses were performed by RT-PCR. RSV-positive amplicons were sequenced and analyzed for genotype assignment.
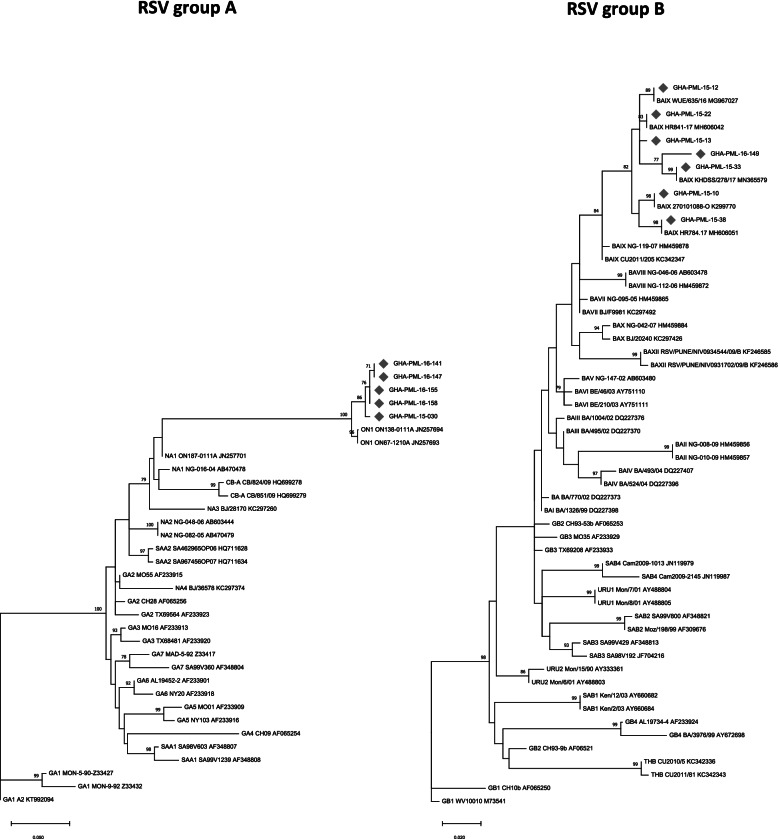
Results: RSV and HMPV prevalence among the sampled subjects were 11.4 and 1.7% respectively. Of the RSV positives, 8/20 (40%) were RSV-A and 12/20 (60%) were RSV-B. The highest prevalence was observed in children less than 12 months old. Phylogenetic analysis of the second hypervariable region of the RSV G-gene revealed that all RSV group A viruses belonged to the "novel" ON1 genotype containing the 72-nucleotide duplication; and RSV group B viruses belong to the BA IX genotype.
Conclusion: RSV is frequently detected in children aged under 5 years admitted with ALRTI in Ghana. Continued surveillance of viral aetiological agents is warranted to elucidate the prevalence and transmission patterns of viral pathogens that cause respiratory tract infections among children. This will help inform appropriate intervention approaches.
Keywords: ALRTI; Children; Ghana; HMPV; Molecular epidemiology; RSV.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- O’Brien KL, Baggett HC, Brooks WA, Feikin DR, Hammitt LL, Higdon MM, Howie SRC, Deloria Knoll M, Kotloff KL, Levine OS, et al. Causes of severe pneumonia requiring hospital admission in children without HIV infection from Africa and Asia: the PERCH multi-country case-control study. Lancet. 2019;394(10200):757–779. doi: 10.1016/S0140-6736(19)30721-4. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
