

Development and validation of an ultrasound-based prediction model for differentiating between malignant and benign solid pancreatic lesions
- PMID: 35751698
- PMCID: PMC9705429
- DOI: 10.1007/s00330-022-08930-0
Development and validation of an ultrasound-based prediction model for differentiating between malignant and benign solid pancreatic lesions
Abstract
Objective: To identify the diagnostic ability of precontrast and contrast-enhanced ultrasound (CEUS) in differentiating between malignant and benign solid pancreatic lesions (MSPLs and BSPLs) and to develop an easy-to-use diagnostic nomogram.
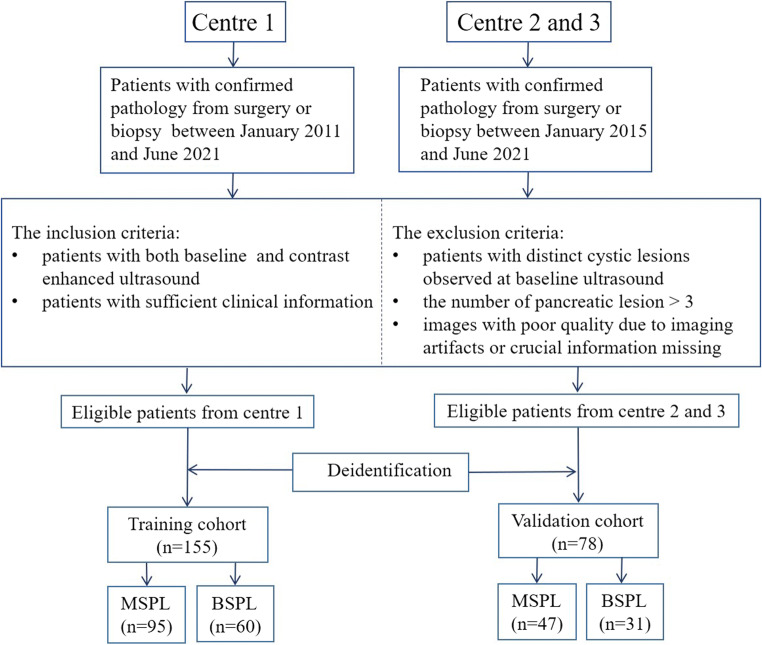
Materials and methods: This study was approved by the institutional review board. Patients with pathologically confirmed solid pancreatic lesions were enrolled from one tertiary medical centre from March 2011 to June 2021 and in two tertiary institutions between January 2015 and June 2021. A prediction nomogram model was established in the training set by using precontrast US and CEUS imaging features that were independently associated with MSPLs. The performance of the prediction model was further externally validated.
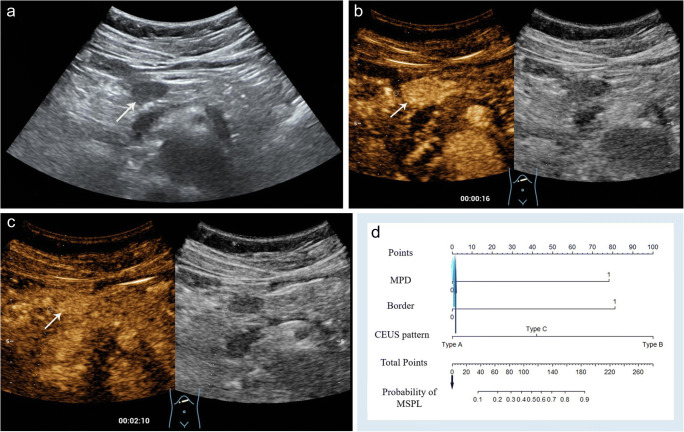
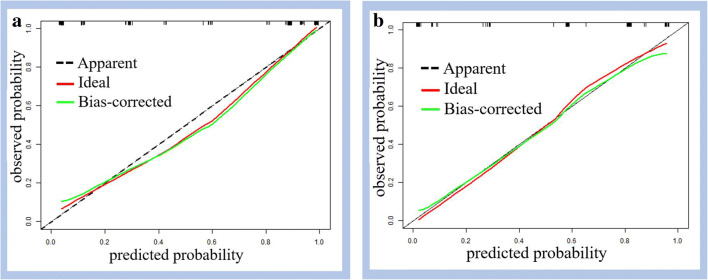
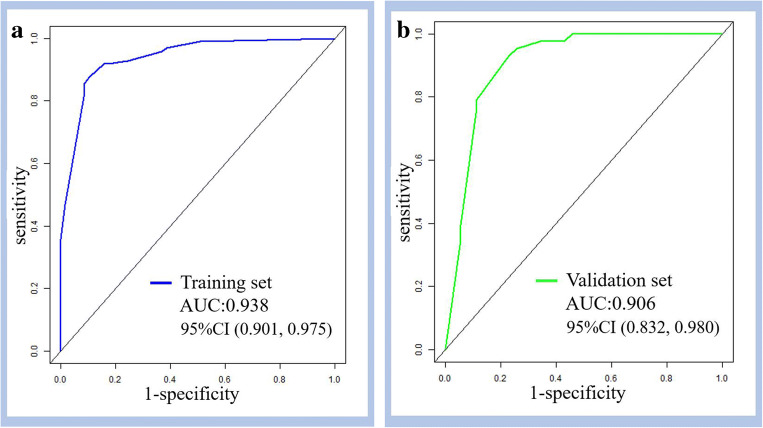
Results: A total of 155 patients (mean age, 55 ± 14.6 years, M/F = 84/71) and 78 patients (mean age, 59 ± 13.4 years, M/F = 36/42) were included in the training and validation cohorts, respectively. In the training set, an ill-defined border and dilated main pancreatic duct on precontrast ultrasound, CEUS patterns of hypoenhancement in both the arterial and venous phases of CEUS, and hyperenhancement/isoenhancement followed by washout were independently associated with MSPLs. The prediction nomogram model developed with the aforementioned variables showed good performance in differentiating MSPLs from BSPLs with an area under the curve (AUC) of 0.938 in the training set and 0.906 in the validation set.
Conclusion: Hypoenhancement in all phases, hyperenhancement/isoenhancement followed by washout on CEUS, an ill-defined border, and a dilated main pancreatic duct were independent risk factors for MSPLs. The nomogram constructed based on these predictors can be used to diagnose MSPLs.
Key points: • An ill-defined border and dilated main pancreatic duct on precontrast ultrasound, hypoenhancement in all phases of CEUS, and hyperenhancement/isoenhancement followed by washout were independently associated with MSPLs. • The ultrasound-based prediction model showed good performance in differentiating MSPLs from BSPLs with an AUC of 0.938 in the training set and 0.906 in the external validation set. • An ultrasound-based nomogram is an easy-to-use tool to differentiate between MSPLs and BSPLs with high efficacy.
Keywords: Contrast media; Nomograms; Pancreatic neoplasms; Ultrasonography.
© 2022. The Author(s).
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article.
Figures


References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
