

Azithromycin use increases the risk of sudden cardiac death in patients with hemodialysis-dependent kidney failure
- PMID: 35752324
- PMCID: PMC9509424
- DOI: 10.1016/j.kint.2022.05.024
Azithromycin use increases the risk of sudden cardiac death in patients with hemodialysis-dependent kidney failure
Abstract
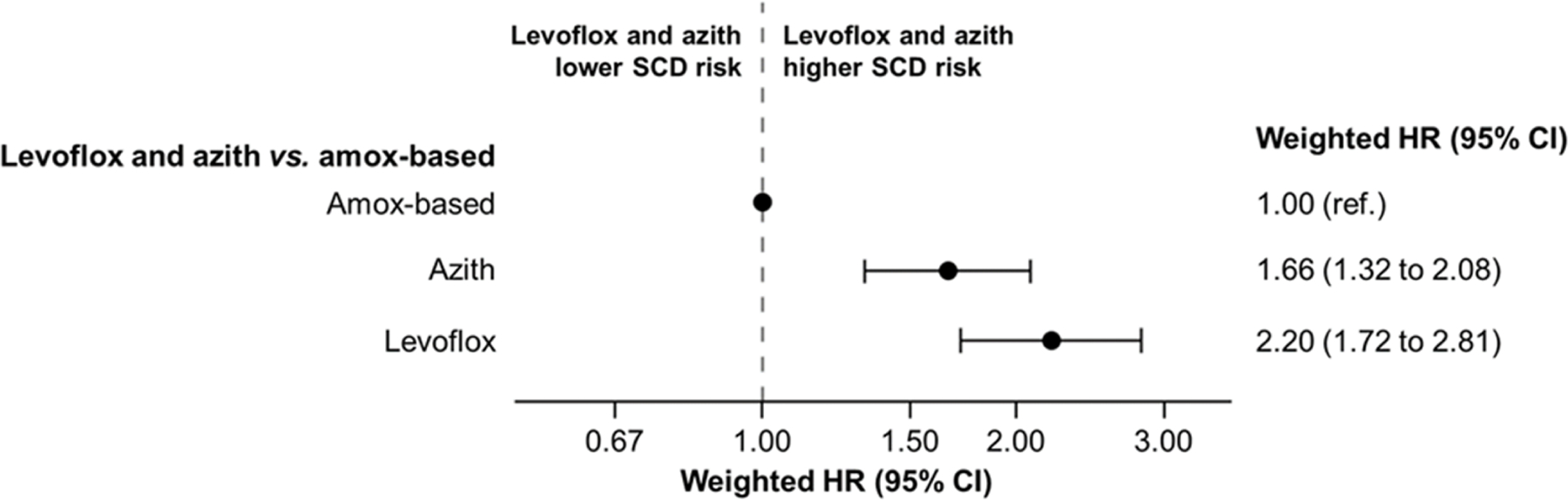
Azithromycin is an antibiotic with QT-prolonging potential commonly prescribed to individuals receiving hemodialysis. Hemodialysis patients have a high prevalence of clinical conditions, such as structural heart disease, that can enhance the pro-arrhythmic effects azithromycin, but were excluded from prior investigations evaluating the cardiac safety of azithromycin. Using data from the United States Renal Data System (2007-2017), we conducted two cohort studies to examine the cardiac safety of azithromycin relative to amoxicillin-based antibiotics (amoxicillin, amoxicillin/clavulanic acid) and levofloxacin (a fluoroquinolone antibiotic known to prolong the QT-interval) in the hemodialysis population. The primary outcome was five-day sudden cardiac death. Using inverse probability of treatment weighted survival models, we estimated hazard ratios, risk differences, and 95% confidence intervals. The azithromycin vs. amoxicillin-based antibiotic cohort included 282,899 patients and 725,431 treatment episodes (381,306 azithromycin and 344,125 amoxicillin-based episodes). Azithromycin vs. amoxicillin-based antibiotic treatment was associated with higher relative and absolute risks of sudden cardiac death, weighted hazard ratio of 1.70 (95% Confidence Interval, 1.36 to 2.11) and weighted risk difference per 100,000 treatment episodes of 25.0 (15.5 to 36.5). The azithromycin vs. levofloxacin cohort included 245,143 patients and 554,557 treatment episodes (387,382 azithromycin and 167,175 levofloxacin episodes). Azithromycin vs. levofloxacin treatment was associated with lower relative and absolute risks of sudden cardiac death, weighted hazard ratio of 0.79 (0.64 to 0.96) and weighted risk difference per 100,000 treatment episodes of -18.9 (-35.5 to -3.8). Thus, when selecting among azithromycin, levofloxacin, and amoxicillin-based antibiotics, clinicians should weigh the relative antimicrobial benefits of these drugs against their potential cardiac risks.
Keywords: USRDS; amoxicillin; azithromycin; hemodialysis; levofloxacin; sudden cardiac death.
Copyright © 2022 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures



Comment in
-
Infection indication and severity.Kidney Int. 2022 Nov;102(5):1191. doi: 10.1016/j.kint.2022.08.010. Kidney Int. 2022. PMID: 36272743 Free PMC article. No abstract available.
References
-
- Chou HW, Wang JL, Chang CH, et al. Risks of cardiac arrhythmia and mortality among patients using new-generation macrolides, fluoroquinolones, and beta-lactam/beta-lactamase inhibitors: a Taiwanese nationwide study. Clin Infect Dis 2015; 60: 566–577. - PubMed
-
- United States Renal Data System. 2020. USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
