

Characterization of the PF-ILD phenotype in patients with advanced pulmonary sarcoidosis
- PMID: 35752806
- PMCID: PMC9233403
- DOI: 10.1186/s12931-022-02094-7
Characterization of the PF-ILD phenotype in patients with advanced pulmonary sarcoidosis
Abstract
Background: Advanced pulmonary sarcoidosis causes significant morbidity and can lead to death. Large trials demonstrated efficacy of antifibrotics in patients with progressive fibrosing interstitial lung diseases (PF-ILD), including a few with sarcoidosis. To date, little is known about this progressive fibrosing phenotype in sarcoidosis. Diffusion capacity of carbon monoxide (DLCO) may be a useful functional marker to screen for advanced pulmonary sarcoidosis. In this study, we describe a cohort with advanced pulmonary sarcoidosis and we gain insights in the progressive fibrosing phenotype in sarcoidosis.
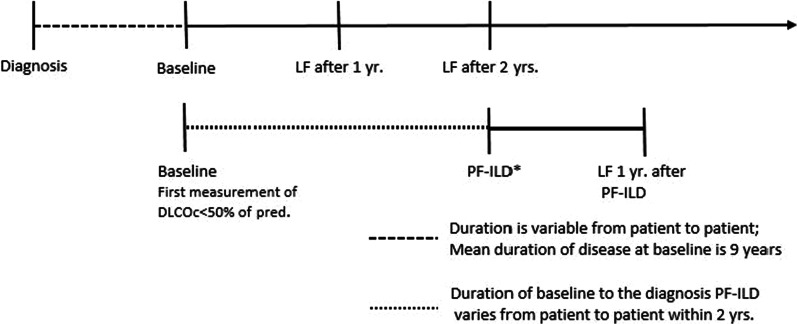
Methods: Patients with sarcoidosis and a DLCO < 50% predicted were included in this retrospective cohort study. First measurement of DLCO < 50% predicted was the baseline. Lung function data, HRCT, pulmonary hypertension (PH) and mortality were collected. Patients with > 10% fibrosis on HRCT meeting the criteria for ILD-progression within 24 months were labelled as PF-ILD. With Cox-regression analysis predictors of mortality were established.
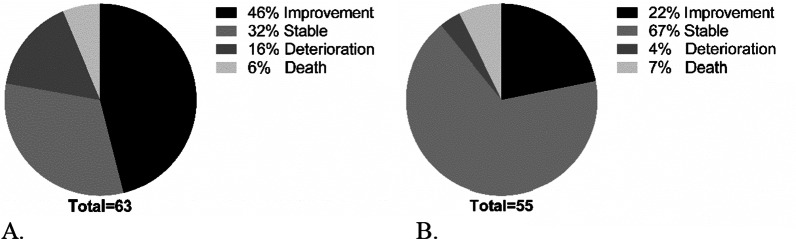
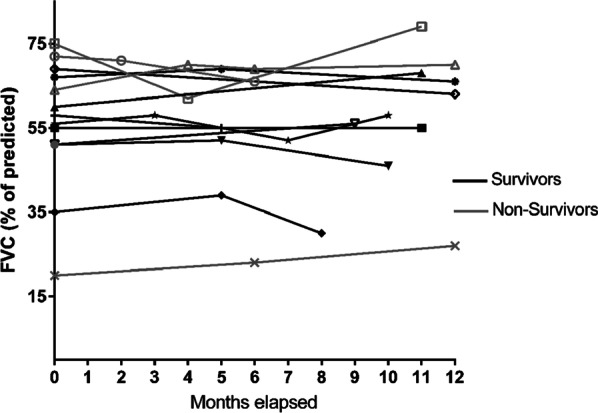
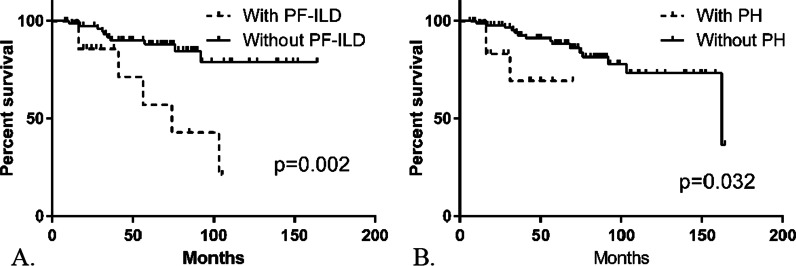
Results: 106 patients with a DLCO < 50% predicted were included. Evolution of forced vital capacity (FVC) varied widely between patients from - 34% to + 45% after 2 years follow-up, whereas change in DLCO varied between - 11% and + 26%. Fourteen patients (15%) met the PF-ILD criteria, of whom 6 (43%) died within 10 years versus 10 (13%) in the non PF-ILD group (p = 0.006). PH was present 12 (11%), 56 (53%) demonstrated > 10% fibrosis on HRCT. Independent predictors of mortality and lung transplantation in the whole cohort are PH, PF-ILD and UIP-like pattern.
Conclusion: In conclusion, within this group with advanced pulmonary sarcoidosis disease course varied widely from great functional improvement to death. PF-ILD patients had higher mortality rate than the mortality in the overall pulmonary sarcoidosis group. Future research should focus on the addition of antifibrotics in these patients. Trial registration retrospectively registered.
Keywords: Advanced sarcoidosis; Diffusion capacity; Mortality; PF-ILD.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
