

A direct referencing method of the tibial plateau for the posterior tibial slope in medial unicompartmental knee arthroplasty
- PMID: 35752859
- PMCID: PMC9233832
- DOI: 10.1186/s13018-022-03179-1
A direct referencing method of the tibial plateau for the posterior tibial slope in medial unicompartmental knee arthroplasty
Abstract
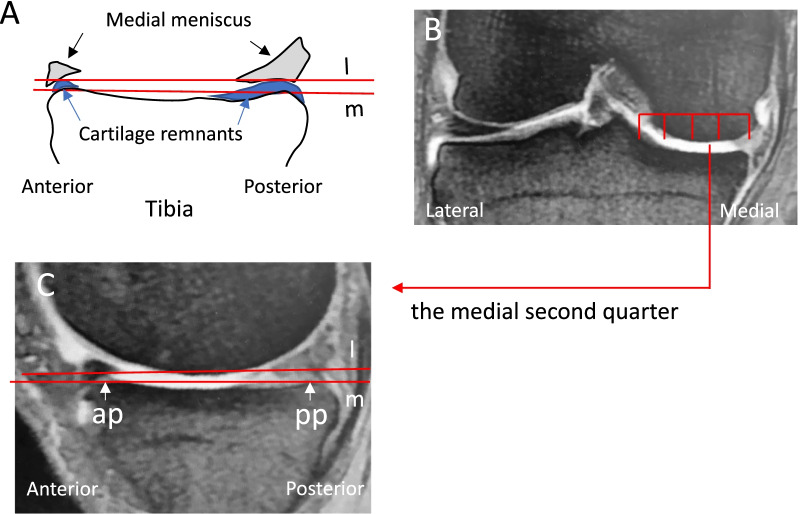
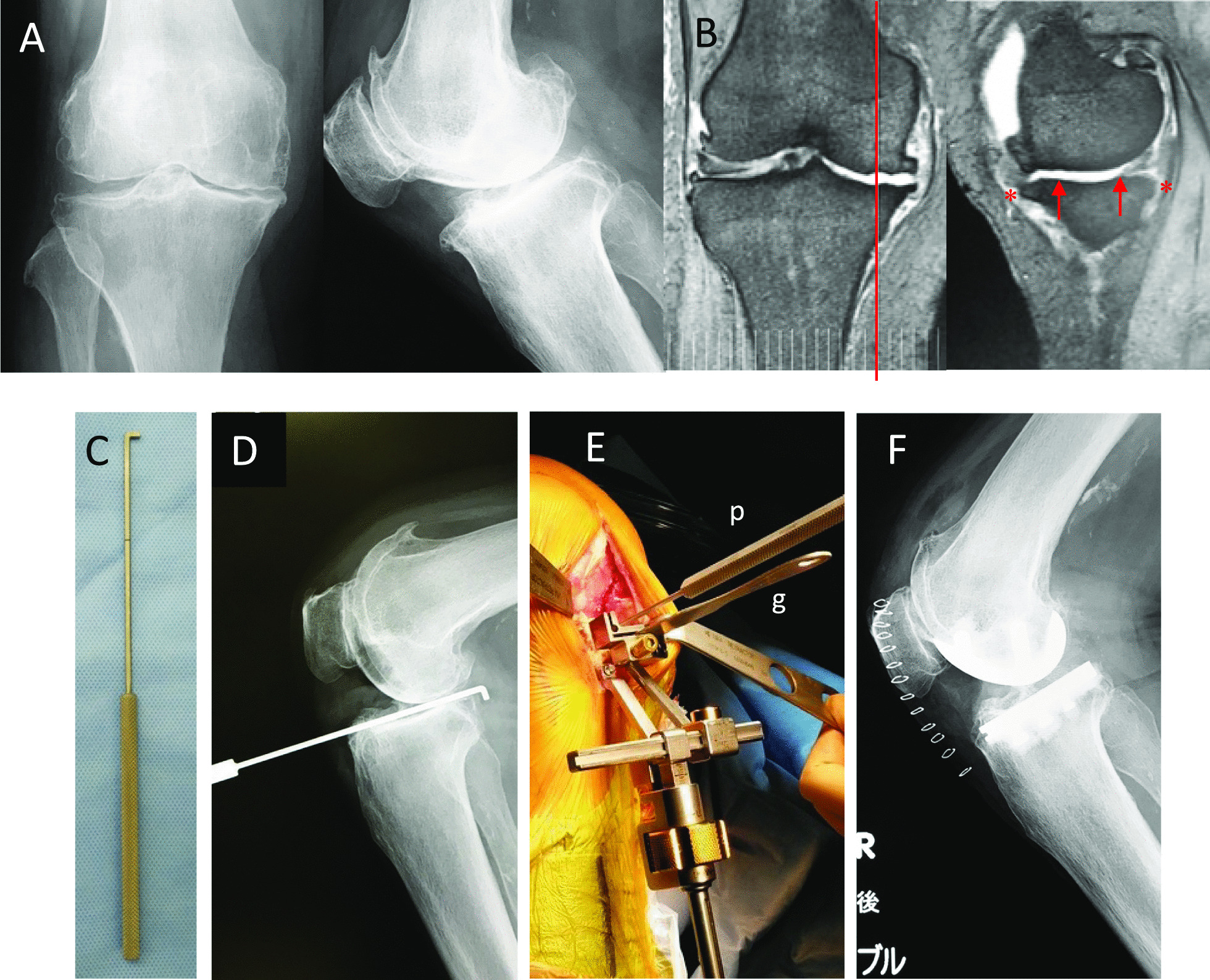
Purpose: There is no consensus on intraoperative references for the posterior tibial slope (PTS) in medial unicompartmental knee arthroplasty (UKA). An arthroscopic hook probe placed on the medial second quarter of the medial tibial plateau (MTP) in an anteroposterior direction may be used as a direct anatomical reference for the PTS. The purpose of this study is to investigate the availability and accuracy of this method.
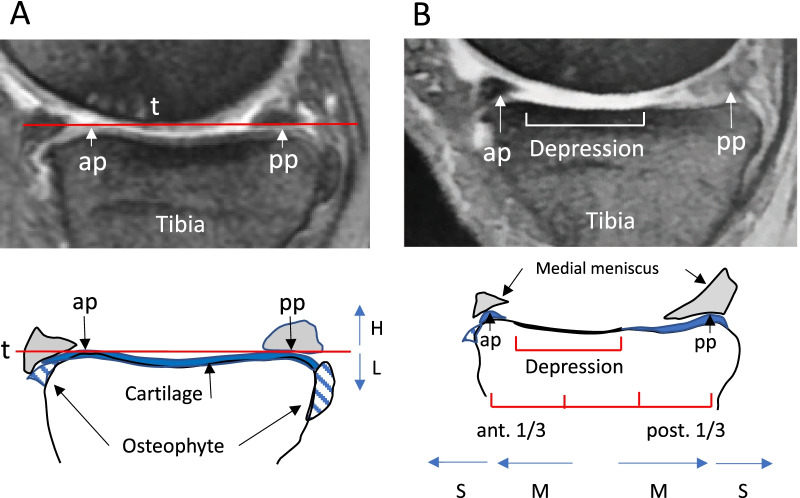
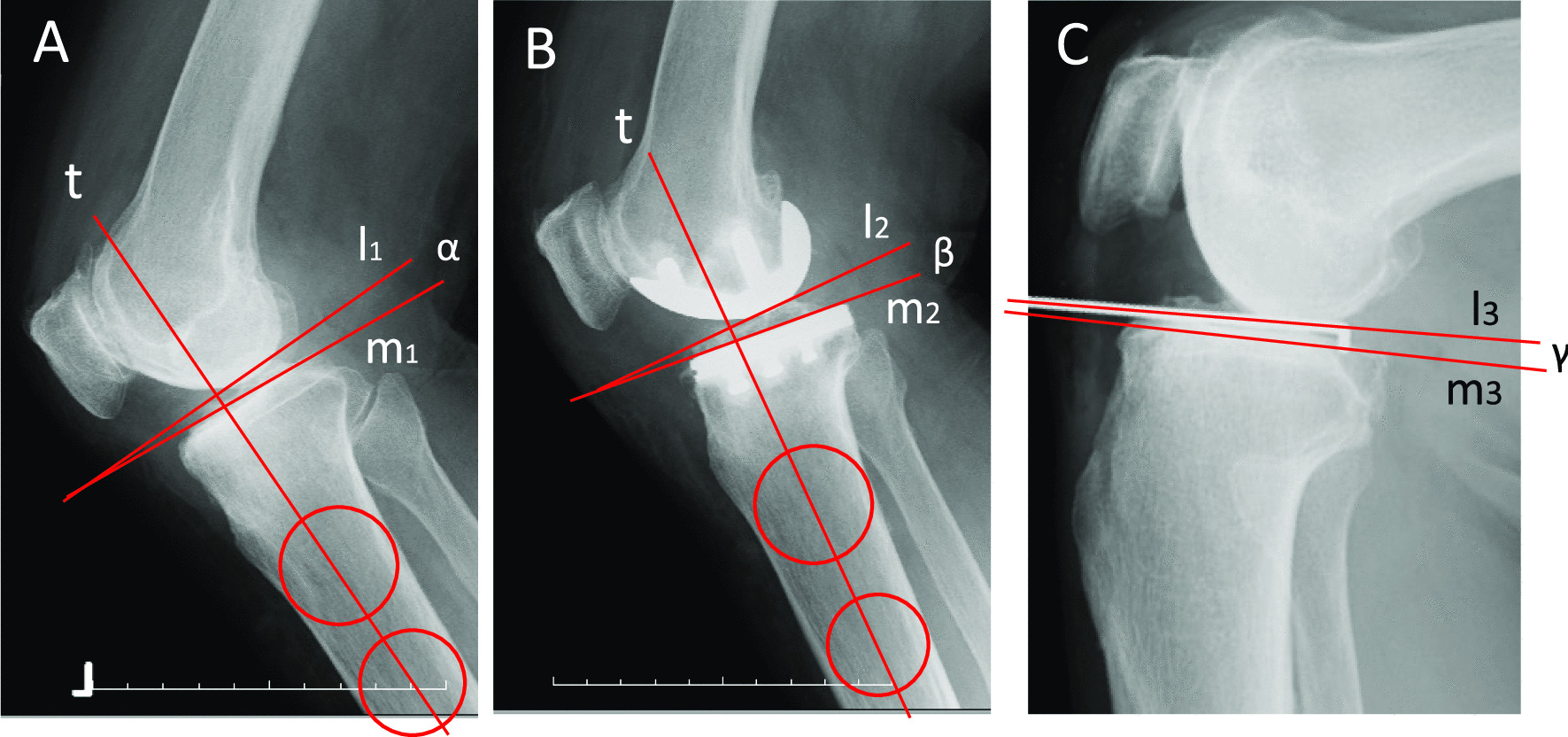
Methods: Marginal osteophyte formation and subchondral depression of the MTP and angles between the bony MTP and the cartilage MTP were retrospectively evaluated using preoperative sagittal MRI of 73 knees undergoing medial UKA. In another 36 knees, intraoperative lateral knee radiographs with the probe placed on the MTP were prospectively taken in addition to the preoperative MRI. Then, angles between the bony MTP and the probe axis and angles between the preoperative bony MTP and the postoperative implant MTP were measured.
Results: Among 73 knees, one knee with grade 4 osteoarthritis had a posterior osteophyte higher than the most prominent point of the cartilage MTP. No subchondral depression affected the direct reference of the MTP. The mean angle between the bony MTP and the cartilage MTP was -0.8° ± 0.7° (-2.6°-1.0°, n = 72), excluding one knee with a "high" osteophyte. The mean angle between the bony MTP and the probe axis on the intraoperative radiograph was -0.6° ± 0.4° (-1.7-0.0, n = 36). The mean angle between the pre- and postoperative MTP was -0.5° ± 1.5° (-2.9°-1.8°). The root-mean-square (RMS) error of these two PTS angles was 1.6° with this method.
Conclusion: Cartilage remnants, osteophyte formation and subchondral bone depression do not affect the direct referencing method in almost all knees for which medial UKA is indicated. When the posterior "high" osteophyte of the MTP is noted on preoperative radiography, preoperative MRI or CT scan is recommended to confirm no "high" osteophyte on the medial second quarter. The accuracy of this method seems equal to that of robotic-assisted surgery (the RMS error in previous reports, 1.6°-1.9°).
Keywords: A direct referencing method; Accuracy; Availability; Medial tibial plateau; Medial unicompartmental knee arthroplasty; Posterior tibial slope.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures



Similar articles
-
Referencing the Tibial Plateau With a Probe Improves the Accuracy of the Posterior Slope in Medial Unicompartmental Knee Arthroplasty.Arthroplast Today. 2022 Oct 22;18:89-94. doi: 10.1016/j.artd.2022.08.017. eCollection 2022 Dec. Arthroplast Today. 2022. PMID: 36312887 Free PMC article.
-
The Medial Tibial Plateau Can Be Used as a Direct Anatomical Reference for the Posterior Tibial Slope in Medial Unicompartmental Knee Arthroplasty.J Knee Surg. 2023 Apr;36(5):555-561. doi: 10.1055/s-0041-1740384. Epub 2021 Dec 17. J Knee Surg. 2023. PMID: 34921377
-
Better accuracy and implant survival in medial imageless robotic-assisted unicompartmental knee arthroplasty compared to conventional unicompartmental knee arthroplasty: two- to eleven-year follow-up of three hundred fifty-six consecutive knees.Int Orthop. 2023 Feb;47(2):533-541. doi: 10.1007/s00264-022-05640-6. Epub 2022 Nov 24. Int Orthop. 2023. PMID: 36434294
-
An Experienced Surgeon Can Meet or Exceed Robotic Accuracy in Manual Unicompartmental Knee Arthroplasty.J Bone Joint Surg Am. 2019 Aug 21;101(16):1479-1484. doi: 10.2106/JBJS.18.00906. J Bone Joint Surg Am. 2019. PMID: 31436656
-
[Research progress on finite element analysis of unicompartmental knee arthroplasty in medial knee compartmental osteoarthritis].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021 Jun 15;35(6):781-785. doi: 10.7507/1002-1892.202101028. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2021. PMID: 34142508 Free PMC article. Review. Chinese.
Cited by
-
Referencing the Tibial Plateau With a Probe Improves the Accuracy of the Posterior Slope in Medial Unicompartmental Knee Arthroplasty.Arthroplast Today. 2022 Oct 22;18:89-94. doi: 10.1016/j.artd.2022.08.017. eCollection 2022 Dec. Arthroplast Today. 2022. PMID: 36312887 Free PMC article.
References
-
- Campi S, Pandit H, Hooper G, Snell D, Jenkins C, Dodd CAF, Maxwell R, Murray DW. Ten-year survival and seven-year functional results of cementless Oxford unicompartmental knee replacement: a prospective consecutive series of our first 1000 cases. Knee. 2018;25:1231–1237. doi: 10.1016/j.knee.2018.07.012. - DOI - PubMed
-
- Fabre-Aubrespy M, Ollivier M, Pesenti S, Parratte S, Argenson JN. Unicompartmental knee arthroplasty in patients older than 75 results in better clinical outcomes and similar survivorship compared to total knee arthroplasty. A matched controlled study. J Arthroplasty. 2016;31:2668–2671. doi: 10.1016/j.arth.2016.06.034. - DOI - PubMed
-
- Siman H, Kamath AF, Carrillo N, Harmsen WS, Pagnano MW, Sierra RJ. Unicompartmental knee arthroplasty vs total knee arthroplasty for medial compartment arthritis in patients older than 75 years: comparable reoperation, revision, and complication rates. J Arthroplasty. 2017;32:1792–1797. doi: 10.1016/j.arth.2017.01.020. - DOI - PubMed
-
- Burn E, Sanchez-Santos MT, Pandit HG, Hamilton TW, Liddle AD, Murray DW, Pinedo-Villanueva R. Ten-year patient-reported outcomes following total and minimally invasive unicompartmental knee arthroplasty: a propensity score-matched cohort analysis. Knee Surg Sports Traumatol Arthrosc. 2018;26:1455–1464. doi: 10.1007/s00167-016-4404-7. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
