

A novel laparoscopic non-resective technique for the management of strangulated Richter's hernia
- PMID: 35753232
- PMCID: PMC9240795
- DOI: 10.1016/j.ijscr.2022.107335
A novel laparoscopic non-resective technique for the management of strangulated Richter's hernia
Abstract
Introduction and importance: The incidence of Richter's hernias has risen in part due to the increment use of laparoscopic surgery. The standard technique to manage a strangulated Richter's hernia is bowel resection with anastomosis. Alternatively, invagination of the necrotic area in the enterocele maintains a clean surgical field and allows for the use of a mesh when closing the abdominal wall. In a sterile surgical field, the use of a prosthetic reinforcement has shown advantages, including low rates of long-term complications and reduced rates of hernia recurrence.
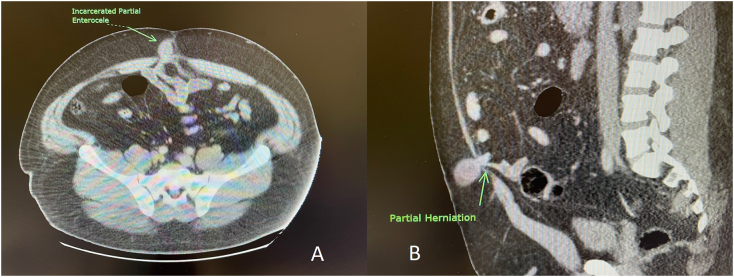
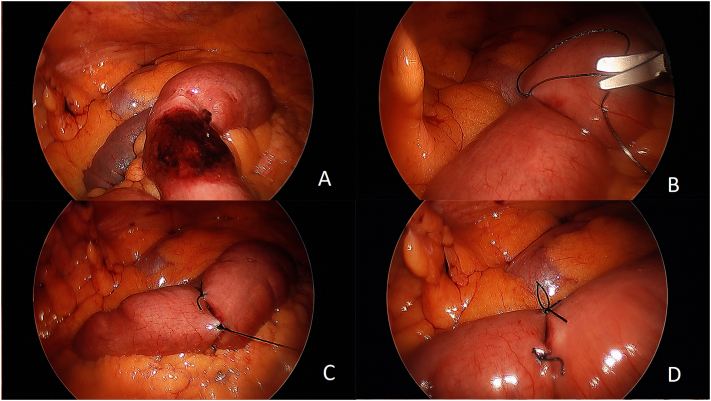
Case presentation: A 35-year-old male presented with a strangulated Richter's hernia in a periumbilical abdominal wall defect. In the Operating Theatre, the necrotic segment was managed laparoscopically by plication with invagination allowing for abdominal wall reconstruction with a mesh.
Clinical discussion and conclusion: We propose the laparoscopic repair of Richter's hernia with plication and invagination whenever feasible, therefore avoiding a bowel resection and maintaining a clean surgical field; which allows for use of prosthetic mesh.
- •
Richter hernias are becoming more common, mostly as a result of port-site closure defects after laparoscopic surgery
- •
Avoiding bowel resection will increase the likelihood of a successful long-term mesh implant and decrease hernia recurrences.
- •
Likewise, avoiding a bowel anastomosis will prevent additional contamination while simplifying the procedure.
Keywords: Case report; Enteroplication; Laparoscopic non-resective technique; Partial enterocele; Richter's hernia.
Conflict of interest statement
The authors (MC and ESS) declare that they have no conflict of interest pertaining to this case report.
Figures
References
-
- Velanovich V. Laparoscopic vs open surgery. Surg. Endosc. 2000 Jan;14(1):16–21. - PubMed
-
- Xourafas D., Lipsitz S.R., Negro P., et al. Impact of mesh use on morbidity following ventral hernia repair with a simultaneous bowel resection. Arch. Surg. 2010;145(8):739–744. - PubMed
-
- Venara A., Hubner M., Le Naoures P., et al. Surgery for incarcerated hernia: short-term outcome with or without mesh. Langenbeck's Arch. Surg. 2014 Jun;399(5):571–577. - PubMed
LinkOut - more resources
Full Text Sources
