

Inhaled nitric oxide: role in the pathophysiology of cardio-cerebrovascular and respiratory diseases
- PMID: 35754072
- PMCID: PMC9234017
- DOI: 10.1186/s40635-022-00455-6
Inhaled nitric oxide: role in the pathophysiology of cardio-cerebrovascular and respiratory diseases
Abstract
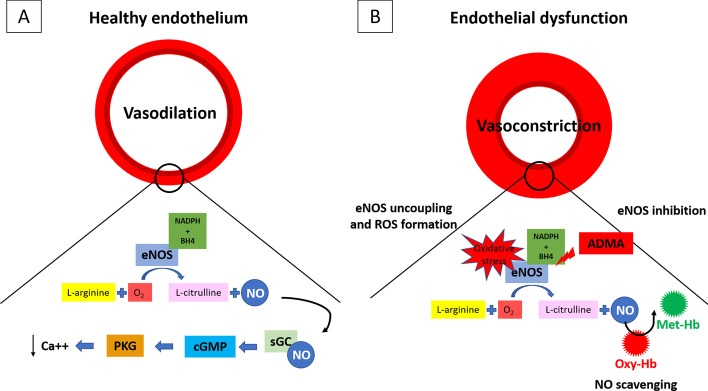
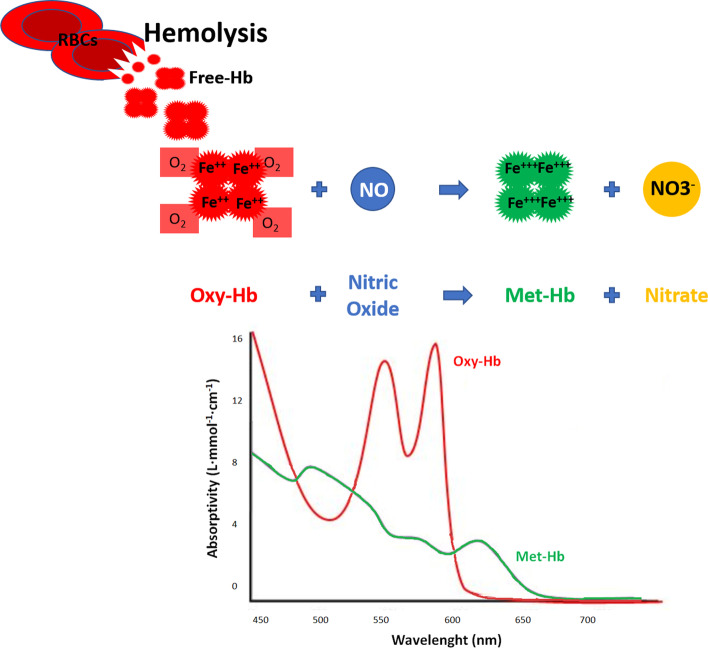
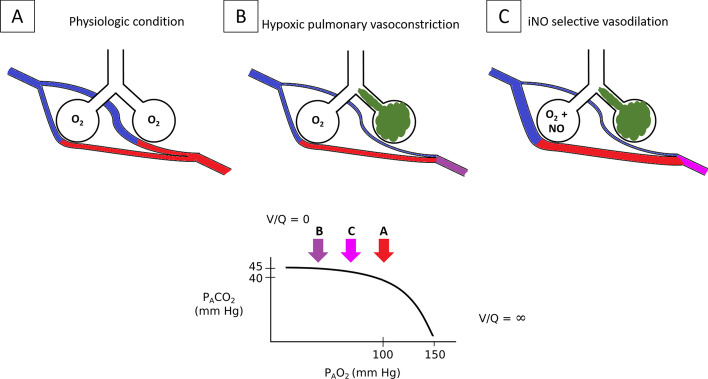
Nitric oxide (NO) is a key molecule in the biology of human life. NO is involved in the physiology of organ viability and in the pathophysiology of organ dysfunction, respectively. In this narrative review, we aimed at elucidating the mechanisms behind the role of NO in the respiratory and cardio-cerebrovascular systems, in the presence of a healthy or dysfunctional endothelium. NO is a key player in maintaining multiorgan viability with adequate organ blood perfusion. We report on its physiological endogenous production and effects in the circulation and within the lungs, as well as the pathophysiological implication of its disturbances related to NO depletion and excess. The review covers from preclinical information about endogenous NO produced by nitric oxide synthase (NOS) to the potential therapeutic role of exogenous NO (inhaled nitric oxide, iNO). Moreover, the importance of NO in several clinical conditions in critically ill patients such as hypoxemia, pulmonary hypertension, hemolysis, cerebrovascular events and ischemia-reperfusion syndrome is evaluated in preclinical and clinical settings. Accordingly, the mechanism behind the beneficial iNO treatment in hypoxemia and pulmonary hypertension is investigated. Furthermore, investigating the pathophysiology of brain injury, cardiopulmonary bypass, and red blood cell and artificial hemoglobin transfusion provides a focus on the potential role of NO as a protective molecule in multiorgan dysfunction. Finally, the preclinical toxicology of iNO and the antimicrobial role of NO-including its recent investigation on its role against the Sars-CoV2 infection during the COVID-19 pandemic-are described.
Keywords: Blood transfusion; Brain disorder; Cardiac arrest; Cardiopulmonary bypass; Endothelial dysfunction; Hemolysis; Ischemia reperfusion; Nitric oxide; Pulmonary hypertension; Shunt; Toxicology.
© 2022. The Author(s).
Conflict of interest statement
The authors have no competing interests to declare.
Figures
References
-
- (1998) Award ceremony speech. NobelPrize.org. In: https://www.nobelprize.org/prizes/medicine/1998/ceremony-speech/
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
