

Progressive Olfactory Impairment and Cardiac Sympathetic Denervation in REM Sleep Behavior Disorder
- PMID: 35754288
- PMCID: PMC9535565
- DOI: 10.3233/JPD-223201
Progressive Olfactory Impairment and Cardiac Sympathetic Denervation in REM Sleep Behavior Disorder
Abstract
Background: Isolated rapid eye movement sleep behavior disorder (iRBD) is prodromal for Parkinson's disease (PD) and dementia with Lewy bodies (DLB).
Objective: We investigated the use of cardiac [123I]meta-iodo-benzyl-guanidine scintigraphy ([123I]MIBG) and olfactory testing- in comparison to [123I]N-ω-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl)nortropane single photon emission computed tomography ([123I]FP-CIT-SPECT)- for identifying iRBD patients as prodromal phenotype of PD/DLB.
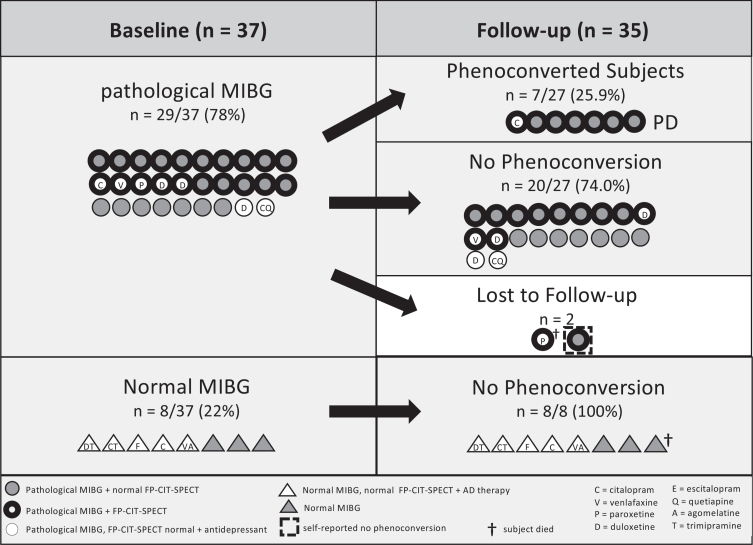
Methods: 37 RBD subjects underwent cardiac [123I]MIBG and brain [123I]FP-CIT-SPECT at baseline. Olfactory (Sniffin' Sticks), cognitive and motor functions were tested annually for ∼4 years.
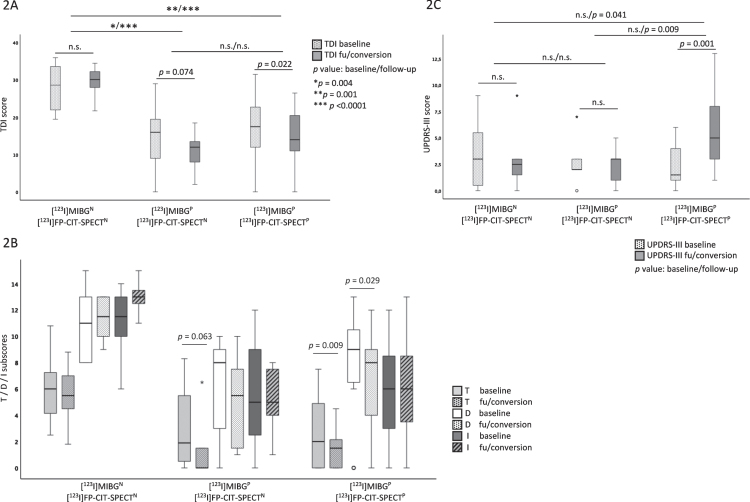
Results: 29/37 (78.4%) subjects had a pathological [123I]MIBG, of whom 86.2% (25/29) presented at least a moderate hyposmia at baseline (threshold/discrimination/identification-(TDI-)score ≤25). 20/37 (54.1%) subjects had a pathological [123I]FP-CIT-SPECT, always combined with a pathological [123I]MIBG. In subjects with pathological [123I]MIBG, olfactory function worsened (mainly due to threshold and discrimination subscores) from baseline to follow-up (p = 0.005). Olfaction was more impaired in subjects with pathological [123I]MIBG compared to those with normal [123I]MIBG at baseline (p = 0.001) and follow-up (p < 0.001). UPDRS-III scores increased in subjects with both pathological [123I]MIBG and [123I]FP-CIT-SPECT. In this group, seven subjects phenoconverted to PD, all- except for one- presented with at least moderate hyposmia at baseline.
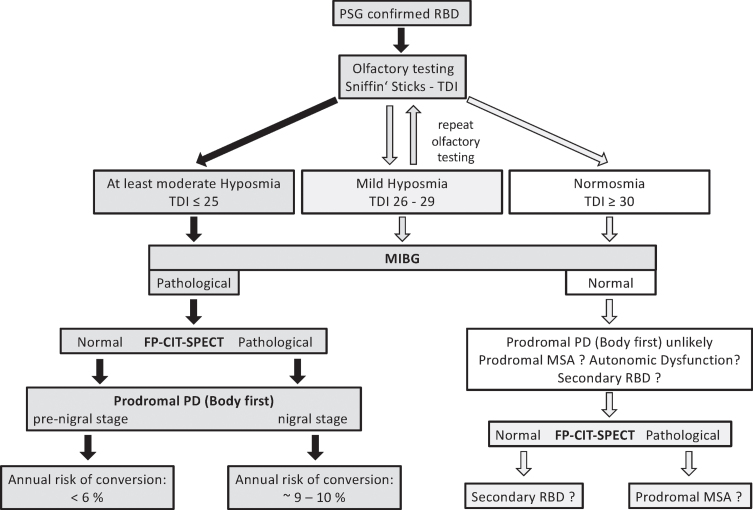
Conclusion: A combination of the biomarkers "pathological [123I]MIBG" and "hyposmia" likely identifies iRBD patients in an early prodromal stage of PD/DLB, i.e., before nigrostriatal degeneration is visualized. One-third of the subjects with pathological [123I]MIBG had a normal [123I]FP-CIT-SPECT. Noteworthy, in iRBD subjects with pathological [123I]MIBG, olfactory impairment is progressive independent of the [123I]FP-CIT-SPECT status.
Keywords: Biomarker; [123I]FP-CIT-SPECT; cardiac [123I]MIBG scintigraphy; hyposmia; isolated rapid eye movement sleep behavior disorder; prodromal progression marker.
Conflict of interest statement
Annette Janzen, MD, reports grants from ParkinsonFonds Deutschland outside the submitted work. David Vadasz, MD, reports no competing interests. Jan Booij, MD, PhD, is consultant at GE healthcare (all paid to the institution). Markus Luster, MD, reports no competing interests. Damiano Librizzi, MD, reports no competing interests. Martin T. Henrich, MD, reports grants from the ParkinsonFonds Deutschland and the German Society for Parkinson and Movement Disorders outside the submitted work. Lars Timmermann, MD, received payments as a consultant for Boston Scientific between September 2018 and September 2021 and received honoraria as a speaker on symposia sponsored by UCB, Desitin, Boston Scientific, AbbVie, Novartis, GlaxoSmithKline, and DIAPLAN. The institution of L.T., not L.T. personally, received funding from Boston Scientific, the German Research Foundation, the German Ministry of Education and Research, and the Deutsche Parkinson Vereinigung. Neither Lars Timmermann nor any member of his family holds stocks, stock options, patents, or financial interests in any of the aforementioned companies or their competitors. Mahboubeh Habibi reports no competing interests. Elisabeth Sittig reports no competing interests. Geert Mayer, MD, reports no competing interests. Fanni F. Geibl, MD, PhD, reports grants from ParkinsonFonds Deutschland and P.E. Kempkes outside the submitted work. Wolfgang H. Oertel, MD, PhD, reports grants from ParkinsonFonds Deutschland, grants from Michael J Fox Foundation, grants from Deutsche Forschungsgemeinschaft (DFG), during the conduct of the study; personal fees from Adamas, MODAG, Roche and UCB; outside the submitted work. WHO is Hertie-Senior-Research Professor supported by the Charitable Hertie-Foundation, Frankfurt/Main, Germany.
Figures
References
-
- Postuma RB, Iranzo A, Hu M, Högl B, Boeve BF, Manni R, Oertel WH, Arnulf I, Ferini-Strambi L, Puligheddu M, Antelmi E, Cochen De Cock V, Arnaldi D, Mollenhauer B, Videnovic A, Sonka K, Jung KY, Kunz D, Dauvilliers Y, Provini F, Lewis SJ, Buskova J, Pavlova M, Heidbreder A, Montplaisir JY, Santamaria J, Barber TR, Stefani A, St Louis EK, Terzaghi M, Janzen A, Leu-Semenescu S, Plazzi G, Nobili F, Sixel-Doering F, Dusek P, Bes F, Cortelli P, Ehgoetz Martens K, Gagnon JF, Gaig C, Zucconi M, Trenkwalder C, Gan-Or Z, Lo C, Rolinski M, Mahlknecht P, Holzknecht E, Boeve AR, Teigen LN, Toscano G, Mayer G, Morbelli S, Dawson B, Pelletier A (2019) Risk and predictors of dementia and parkinsonism in idiopathic REM sleep behaviour disorder: A multicentre study. Brain 142, 744–759. - PMC - PubMed
-
- Iranzo A, Santamaria J, Tolosa E (2016) Idiopathic rapid eye movement sleep behaviour disorder: Diagnosis, management, and the need for neuroprotective interventions. Lancet Neurol 15, 405–419. - PubMed
-
- Schenck CH, Mahowald MW (2002) REM sleep behavior disorder: Clinical, developmental, and neuroscience perspectives 16 years after its formal identification in SLEEP. Sleep 25, 120–138. - PubMed
-
- Horsager J, Andersen KB, Knudsen K, Skjærbæk C, Fedorova TD, Okkels N, Schaeffer E, Bonkat SK, Geday J, Otto M, Sommerauer M, Danielsen EH, Bech E, Kraft J, Munk OL, Hansen SD, Pavese N, Göder R, Brooks DJ, Berg D, Borghammer P (2020) Brain-first versus body-first Parkinson’s disease: A multimodal imaging case-control study. Brain 143, 3077–3088. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
