

Epidemiology of native kidney disease in Flanders: results from the FCGG kidney biopsy registry
- PMID: 35756729
- PMCID: PMC9217646
- DOI: 10.1093/ckj/sfac033
Epidemiology of native kidney disease in Flanders: results from the FCGG kidney biopsy registry
Abstract
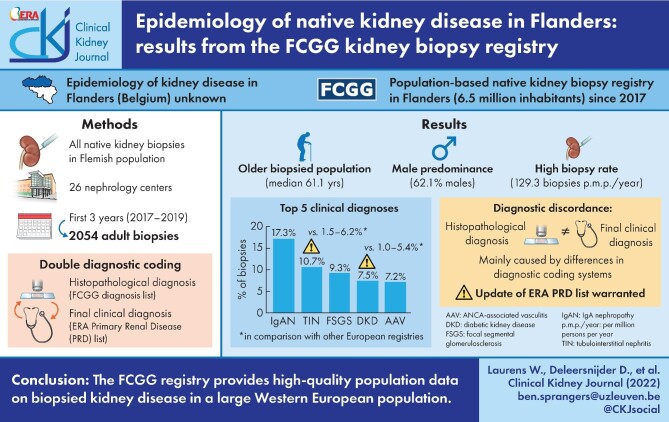
Background: The Flemish Collaborative Glomerulonephritis Group (FCGG) registry is the first population-based native kidney biopsy registry in Flanders, Belgium. In this first analysis, we report on patient demographics, frequency distribution and incidence rate of biopsied kidney disease in adults in Flanders.
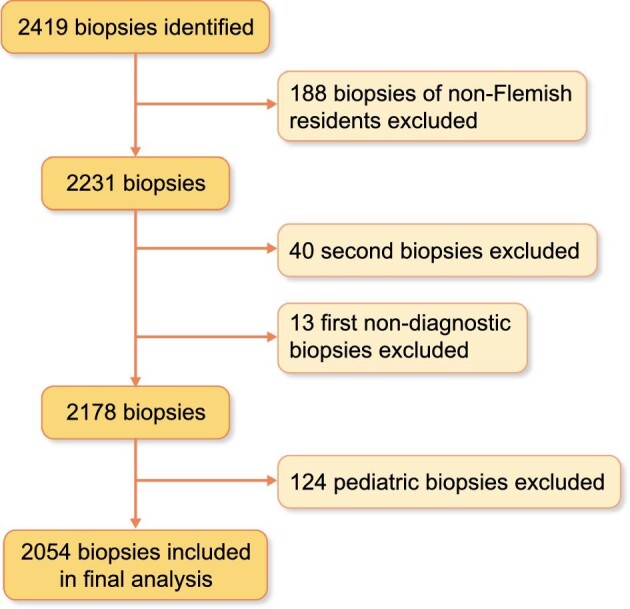
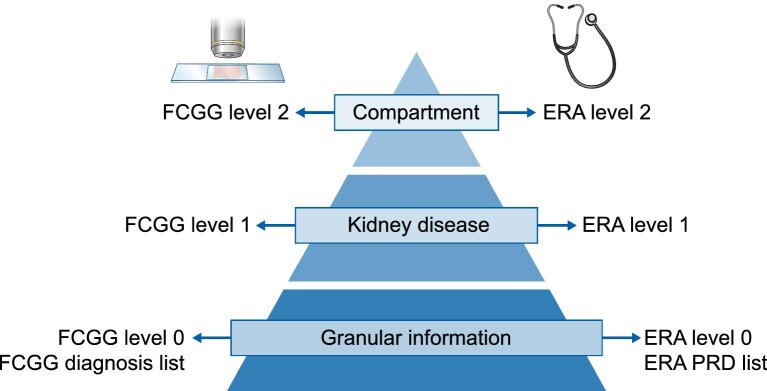
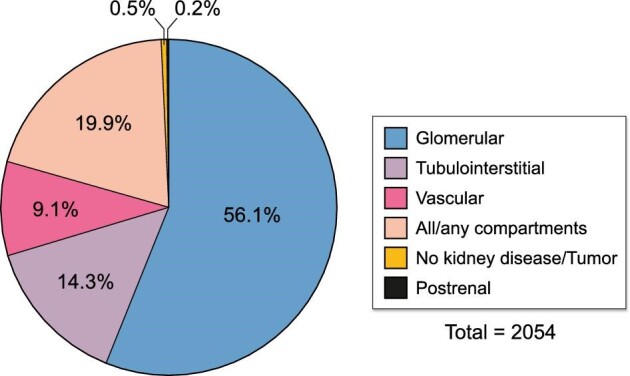
Methods: From January 2017 to December 2019, a total of 2054 adult first native kidney biopsies were included. A 'double diagnostic coding' strategy was used, in which every biopsy sample received a histopathological and final clinical diagnosis. Frequency distribution and incidence rate of both diagnoses were reported and compared with other European registries.
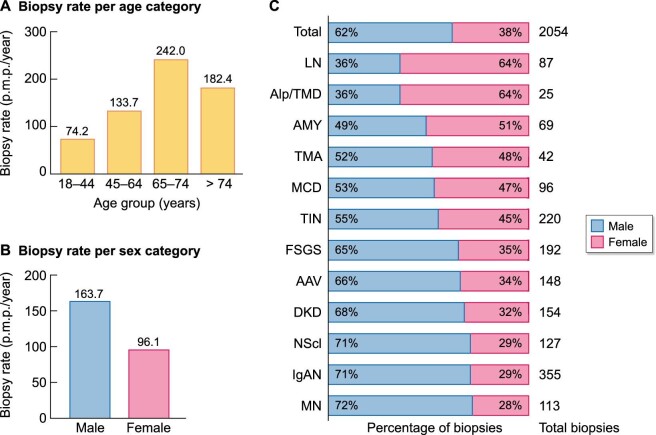
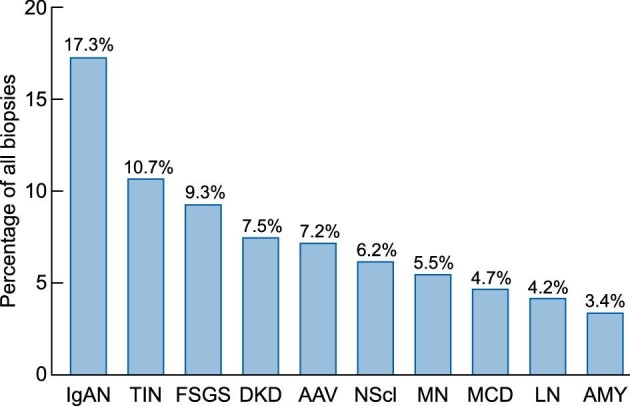
Results: The median age at biopsy was 61.1 years (interquartile range, 46.1-71.7); male patients were more prevalent (62.1%) and biopsy incidence rate was 129.3 per million persons per year. Immunoglobulin A nephropathy was the most frequently diagnosed kidney disease (355 biopsies, 17.3% of total) with a similar frequency as in previously published European registries. The frequency of tubulointerstitial nephritis (220 biopsies, 10.7%) and diabetic kidney disease (154 biopsies, 7.5%) was remarkably higher, which may be attributed to changes in disease incidence as well as biopsy practices. Discordances between histopathological and final clinical diagnoses were noted and indicate areas for improvement in diagnostic coding systems.
Conclusions: The FCGG registry, with its 'double diagnostic coding' strategy, provides useful population-based epidemiological data on a large Western European population and allows subgroup selection for future research.
Keywords: biopsy; epidemiology; frequency; incidence; native kidney; observational; pathology; registry.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures
References
-
- Fiorentino M, Bolignano D, Tesar Vet al. Renal biopsy in 2015—from epidemiology to evidence-based indications. Am J Nephrol 2016; 43: 1–19 - PubMed
LinkOut - more resources
Full Text Sources
