

A real-world study on SGLT2 inhibitors and diabetic kidney disease progression
- PMID: 35756732
- PMCID: PMC9217649
- DOI: 10.1093/ckj/sfac044
A real-world study on SGLT2 inhibitors and diabetic kidney disease progression
Abstract
Background: Randomized controlled trials have demonstrated the benefits of sodium-glucose cotransporter 2 inhibitors (SGLT2is) in people with type 2 diabetes mellitus (T2DM) and chronic kidney disease (CKD). However, real-world data on CKD progression and the development of end-stage kidney disease (ESKD) remains scarce. Our aim was to study renal outcomes of people with diabetic kidney disease (DKD) using SGLT2is in a highly prevalent DKD population.
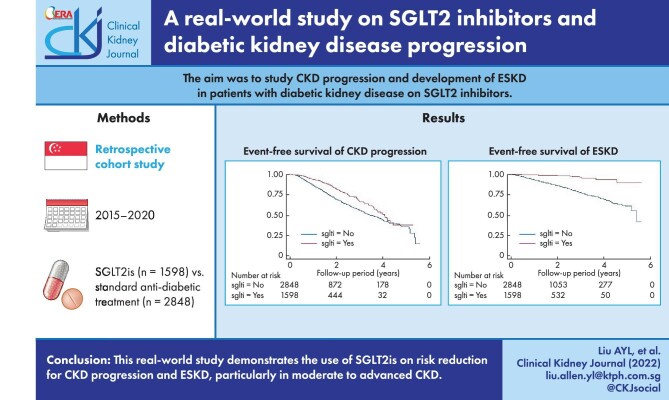
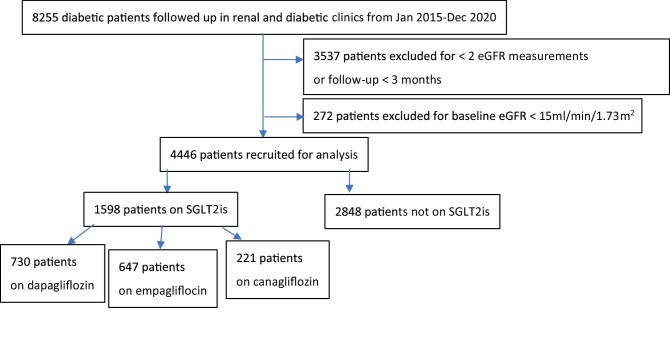
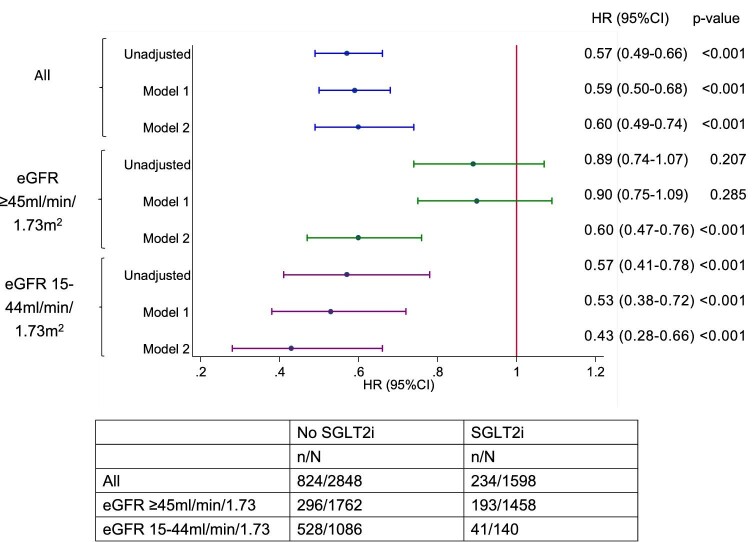
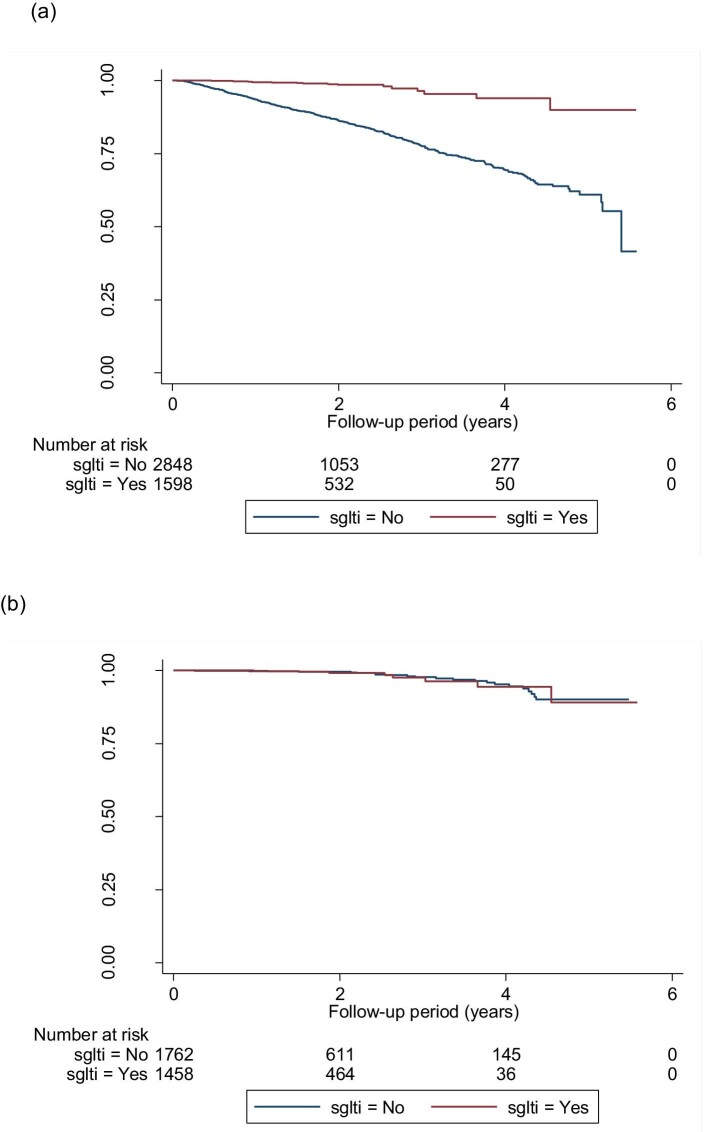
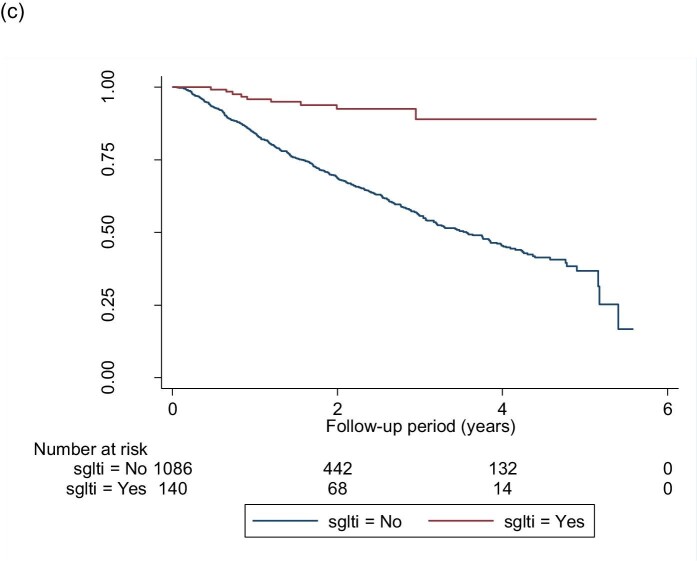
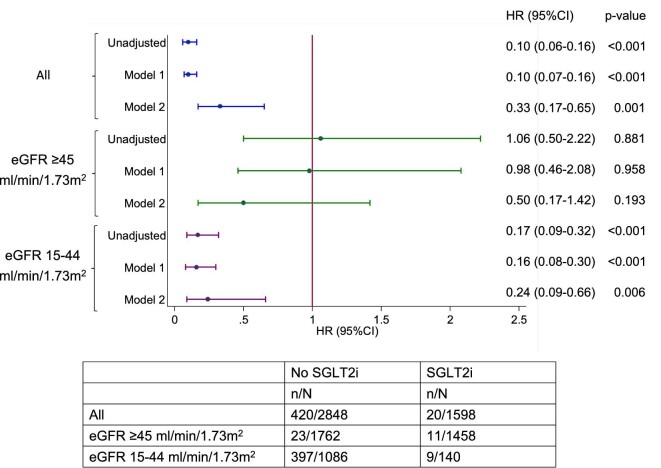
Methods: Between 2016 and 2019 we recruited T2DM patients in the renal and diabetic clinics in a regional hospital in Singapore. Patients prescribed SGLT2is were compared with those on standard anti-diabetic and renoprotective treatment. The outcome measures were CKD progression [a ≥25% decrease from baseline and worsening of estimated glomerular filtration rate (eGFR) categories according to the Kidney Disease: Improving Global Outcomes guidelines] and ESKD (eGFR <15 mL/min/1.73 m2).
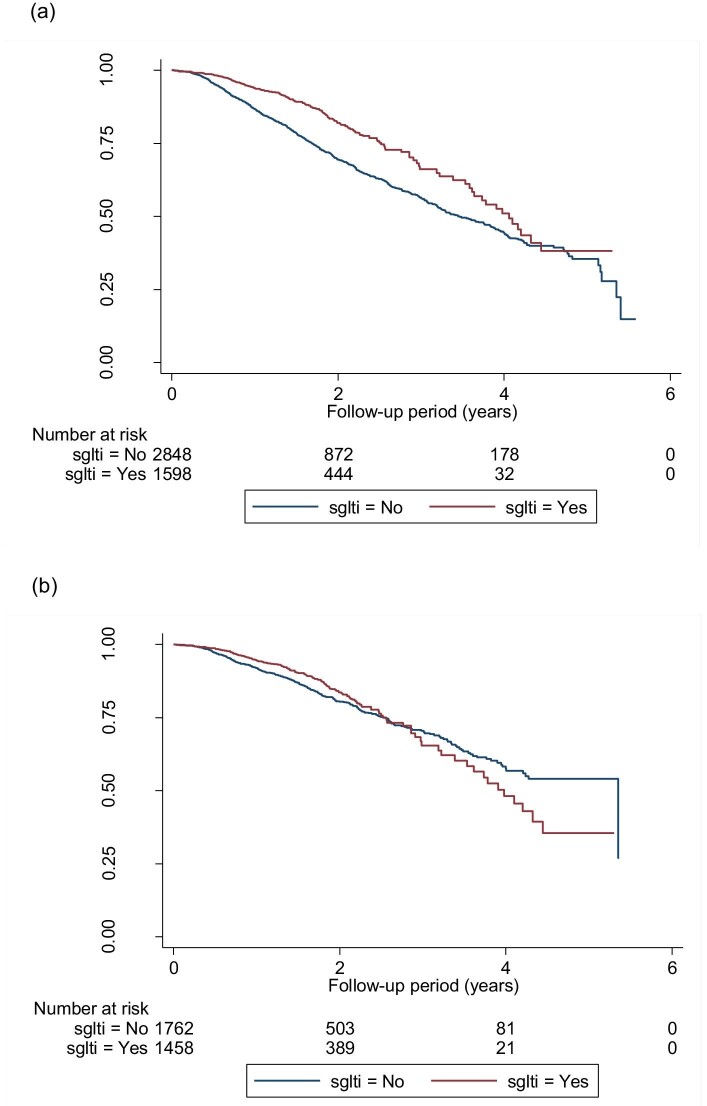
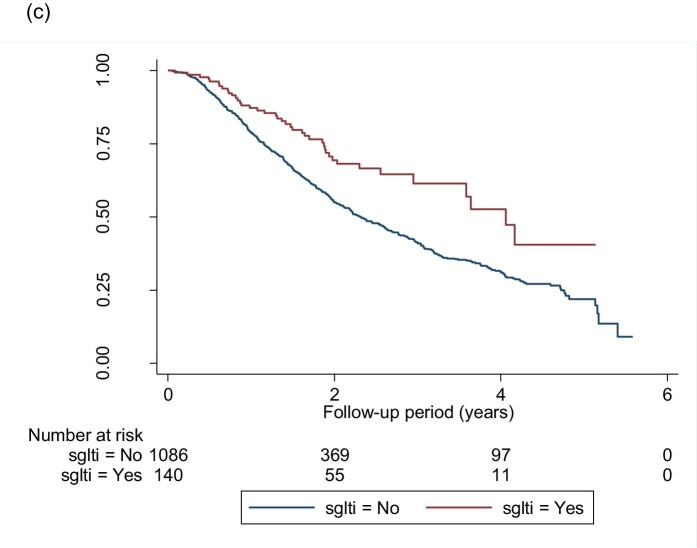
Results: We analysed a total of 4446 subjects; 1598 were on SGLT2is. There was a significant reduction in CKD progression {hazard ratio [HR] 0.60 [95% confidence interval (CI) 0.49-0.74]} with SGLT2is. The HR for eGFR ≥45 mL/min/1.73 m2 and 15-44 mL/min/1.73 m2 was 0.60 (95% CI 0.47-0.76) and 0.43 (95% CI 0.23-0.66), respectively. There was also a reduction in risk for developing ESKD for the entire cohort [HR 0.33 (95% CI 0.17-0.65)] and eGFR 15-44 mL/min/1.73 m2 [HR 0.24 (95% CI 0.09-0.66)]. Compared with canagliflozin and dapagliflozin, empagliflozin showed a sustained risk reduction of renal outcomes across CKD stages 1-4.
Conclusions: This real-world study demonstrates the benefits of SGLT2is on CKD progression and ESKD. The effect is more pronounced in moderate to advanced CKD patients.
Keywords: CKD progression; ESKD; SGLT2is; diabetes mellitus; diabetic kidney disease; real-world study.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Figures
References
-
- Low SK, Sum CF, Yeoh LYet al. Prevalence of chronic kidney disease in adults with type 2 diabetes mellitus. Ann Acad Med Singap 2015; 44: 164–171 - PubMed
-
- Wanner C, Inzucchi SE, Lachin JMet al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med 2016; 375: 323–334 - PubMed
-
- Zinman B, Wanner C, Lachin JMet al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015; 373: 2117–2128 - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
