

Treatment decision of camouflage or surgical orthodontic treatment for skeletal Class III patients based on analysis of masticatory function
- PMID: 35756806
- PMCID: PMC9201536
- DOI: 10.1016/j.jds.2021.09.036
Treatment decision of camouflage or surgical orthodontic treatment for skeletal Class III patients based on analysis of masticatory function
Abstract
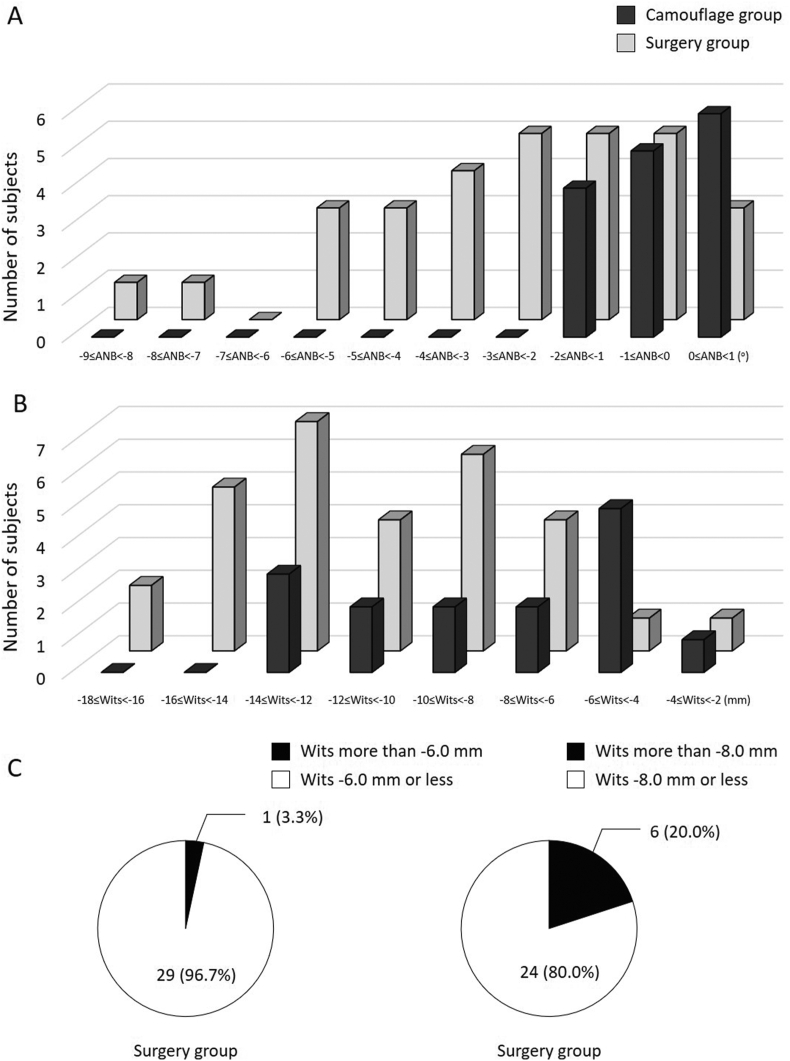
Background/purpose: Surgical orthodontic treatment is recommended for patients with severe dentoskeletal discrepancies, while camouflage orthodontic treatment is recommended for patients with mild to moderate discrepancies. However, the decision as to which treatment should be chosen is complicated. The purpose of this study was to determine differences in masticatory function in patients who underwent camouflage and surgical orthodontic treatment for skeletal Class III malocclusion, as well as the usefulness of Wits appraisal in treatment decision based on masticatory functional analysis.
Materials and methods: The study subjects were 45 patients with skeletal Class III malocclusion (15 cases with camouflage orthodontics and 30 cases with orthognatic surgery) and 12 individuals with normal occlusion. We analyzed the pre-treatment records of electromyographic activities of masseter and temporalis muscles and jaw movements.
Results: There were no significant differences in various functional measurements between the camouflage and surgery groups. However, there were significant but not strong correlations between ANB and both masseter muscle activity (r = 0.36, p < 0.01) and expression ratio of abnormal chewing (r = -0.54, p < 0.01). Division of patients into two groups using a cutoff value of -6.0 mm for Wits appraisal showed a significant difference in masseter muscle activity between -6.0 mm or less group and the control (p < 0.01) but none between more than -6.0 mm group and the control.
Conclusion: Camouflage orthodontic treatment is inappropriate for patients with relatively severe dentoskeletal discrepancies. Wits appraisal of -6.0 mm is a potentially useful parameter for treatment decision.
Keywords: Camouflage orthodontic treatment; Masticatory function; Skeletal class III; Surgical orthodontic treatment; Wits appraisal.
© 2021 Association for Dental Sciences of the Republic of China. Publishing services by Elsevier B.V.
Conflict of interest statement
The authors have no conflicts of interest relevant to this article.
Figures





Similar articles
-
A study of Class III treatment: orthodontic camouflage vs orthognathic surgery.Aust Orthod J. 2015 Nov;31(2):138-48. Aust Orthod J. 2015. PMID: 26999886
-
Treatment decision in adult patients with class III malocclusion: surgery versus orthodontics.Prog Orthod. 2018 Aug 2;19(1):28. doi: 10.1186/s40510-018-0218-0. Prog Orthod. 2018. PMID: 30069814 Free PMC article.
-
Achieving Aesthetics and Function in Class III Malocclusion Through Orthodontic Camouflage: A Clinical Case Report.Cureus. 2024 Jul 21;16(7):e65063. doi: 10.7759/cureus.65063. eCollection 2024 Jul. Cureus. 2024. PMID: 39171007 Free PMC article.
-
Influence of surgical orthodontic treatment on masticatory function in skeletal Class III patients.J Oral Rehabil. 2015 Oct;42(10):733-41. doi: 10.1111/joor.12307. Epub 2015 May 15. J Oral Rehabil. 2015. PMID: 25975774
-
Effects of orthodontic treatment on masticatory muscles activity: a meta-analysis.Ann Hum Biol. 2023 Feb;50(1):465-471. doi: 10.1080/03014460.2023.2271840. Epub 2023 Nov 6. Ann Hum Biol. 2023. PMID: 37929786 Review.
Cited by
-
Position and Dimensions of the Mandibular Condyle in Various Anterior-Posterior Skeletal Patterns: A CBCT Imaging Study in a Sample of Iranian People.Int J Dent. 2024 Dec 27;2024:5895594. doi: 10.1155/ijod/5895594. eCollection 2024. Int J Dent. 2024. PMID: 39759839 Free PMC article.
-
Anterior Tooth Inclination Between Skeletal Class II and III Malocclusions After Surgical Orthodontic Treatment.Diagnostics (Basel). 2025 Jun 18;15(12):1553. doi: 10.3390/diagnostics15121553. Diagnostics (Basel). 2025. PMID: 40564873 Free PMC article.
-
Effect of SEC III protocol on upper airway dimensions in growing class III patients: a retrospective study.BMC Oral Health. 2023 Nov 8;23(1):841. doi: 10.1186/s12903-023-03613-8. BMC Oral Health. 2023. PMID: 37940933 Free PMC article.
References
-
- Kobayashi T., Honma K., Shingaki S., Nakajima T. Changes in masticatory function after orthognathic treatment in patients with mandibular prognathism. Br J Oral Maxillofac Surg. 2001;39:260–265. - PubMed
-
- Nakata Y., Ueda H.M., Kato M., et al. Changes in stomatognathic function induced by orthognathic surgery in patients with mandibular prognathism. J Oral Maxillofac Surg. 2007;65:444–451. - PubMed
-
- Kubota T., Yagi T., Tomonari H., Ikemori T., Miyawaki S. Influence of surgical orthodontic treatment on masticatory function in skeletal Class III patients. J Oral Rehabil. 2015;42:733–741. - PubMed
-
- Ueki K., Marukawa K., Shimada M., Nakagawa K., Yamamoto E., Niizawa S. Changes in the chewing path of patients in skeletal class III with and without asymmetry before and after orthognathic surgery. J Oral Maxillofac Surg. 2005;63:442–448. - PubMed
-
- Takeda H., Nakamura Y., Handa H., Ishii H., Hamada Y., Seto K. Examination of masticatory movement and rhythm before and after surgical orthodontics in skeletal Class III patients with unilateral posterior cross-bite. J Oral Maxillofac Surg. 2009;67:1844–1849. - PubMed
LinkOut - more resources
Full Text Sources
