

Baseline 4D Flow-Derived in vivo Hemodynamic Parameters Stratify Descending Aortic Dissection Patients With Enlarging Aortas
- PMID: 35757320
- PMCID: PMC9218246
- DOI: 10.3389/fcvm.2022.905718
Baseline 4D Flow-Derived in vivo Hemodynamic Parameters Stratify Descending Aortic Dissection Patients With Enlarging Aortas
Abstract
Purpose: The purpose of our study was to assess the value of true lumen and false lumen hemodynamics compared to aortic morphological measurements for predicting adverse-aorta related outcomes (AARO) and aortic growth in patients with type B aortic dissection (TBAD).
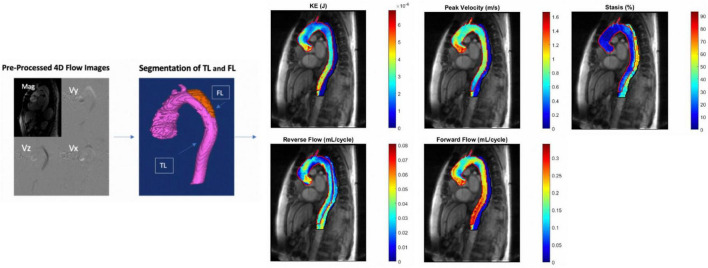
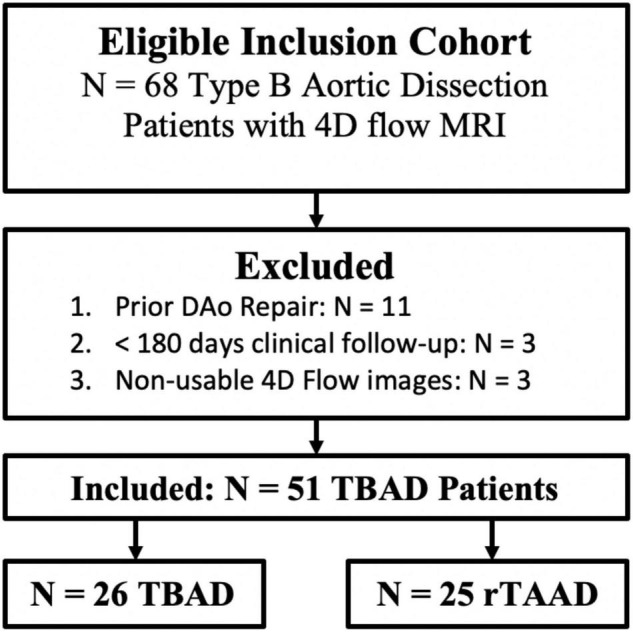
Materials and methods: Using an IRB approved protocol, we retrospectively identified patients with descending aorta (DAo) dissection at a large tertiary center. Inclusion criteria includes known TBAD with ≥ 6 months of clinical follow-up after initial presentation for TBAD or after ascending aorta intervention for patients with repaired type A dissection with residual type B aortic dissection (rTAAD). Patients with prior descending aorta intervention were excluded. The FL and TL of each patient were manually segmented from 4D flow MRI data, and 3D parametric maps of aortic hemodynamics were generated. Groups were divided based on (1) presence vs. absence of AARO and (2) growth rate ≥ vs. < 3 mm/year. True and false lumen kinetic energy (KE), stasis, peak velocity (PV), reverse/forward flow (RF/FF), FL to TL KE ratio, as well as index aortic diameter were compared between groups using the Mann-Whitney U or independent t-test.
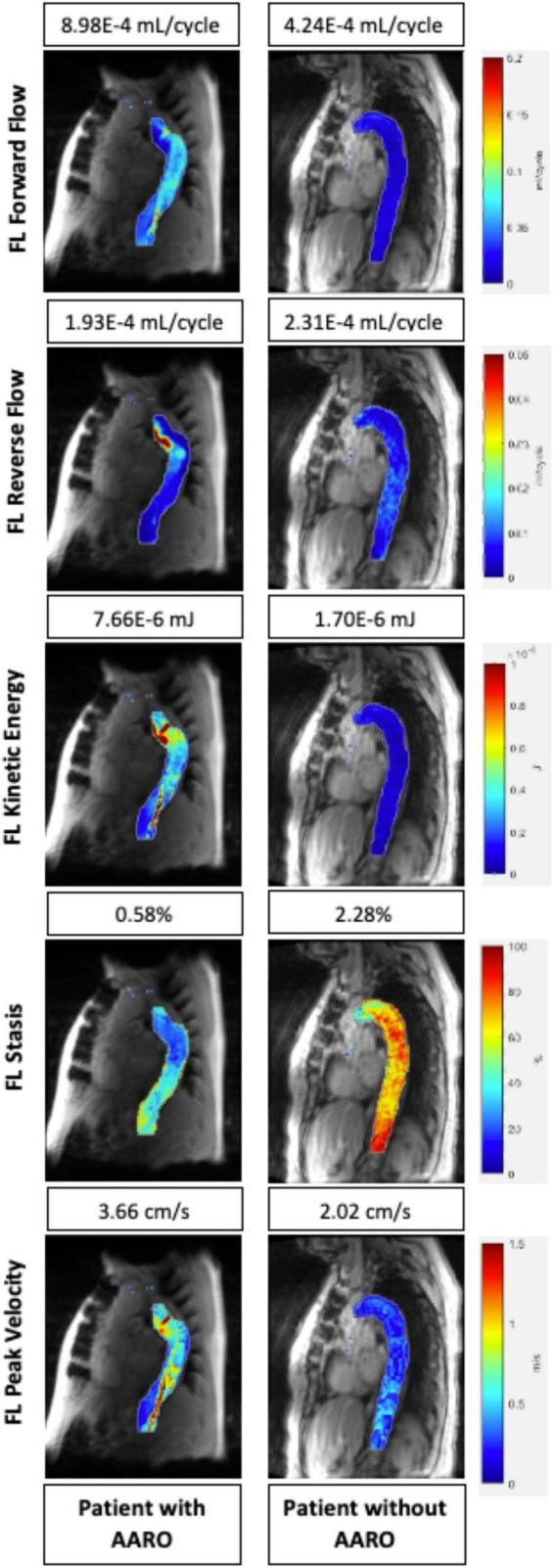
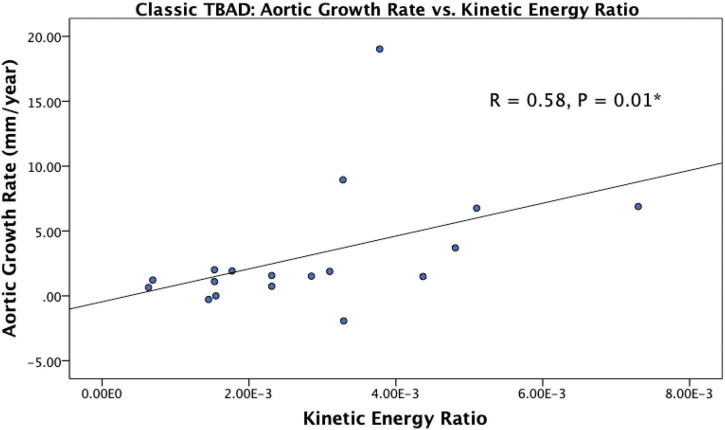
Results: A total of n = 51 patients (age: 58.4 ± 15.0 years, M/F: 31/20) were included for analysis of AARO. This group contained n = 26 patients with TBAD and n = 25 patients with rTAAD. In the overall cohort, AARO patients had larger baseline diameters, lower FL-RF, FL stasis, TL-KE, TL-FF and TL-PV. Among patients with de novo TBAD, those with AAROs had larger baseline diameter, lower FL stasis and TL-PV. In both the overall cohort and in the subgroup of de novo TBAD, subjects with aortic growth ≥ 3mm/year, patients had a higher KE ratio.
Conclusion: Our study suggests that 4D flow MRI is a promising tool for TBAD evaluation that can provide information beyond traditional MRA or CTA. 4D flow has the potential to become an integral aspect of TBAD work-up, as hemodynamic assessment may allow earlier identification of at-risk patients who could benefit from earlier intervention.
Keywords: 4D flow; 4D flow cardiac MRI; CTA (computed tomographic angiography); MRA (magnetic resonance angiography); aortic dissection (AD); cardiac MRI; cardiac MRI (CMR); type B aortic dissection (TBAD).
Copyright © 2022 Chu, Kilinc, Pradella, Weiss, Baraboo, Maroun, Jarvis, Mehta, Malaisrie, Hoel, Carr, Markl and Allen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Interval changes in four-dimensional flow-derived in vivo hemodynamics stratify aortic growth in type B aortic dissection patients.J Cardiovasc Magn Reson. 2024 Winter;26(2):101078. doi: 10.1016/j.jocmr.2024.101078. Epub 2024 Aug 2. J Cardiovasc Magn Reson. 2024. PMID: 39098572 Free PMC article.
-
Parametric Hemodynamic 4D Flow MRI Maps for the Characterization of Chronic Thoracic Descending Aortic Dissection.J Magn Reson Imaging. 2020 May;51(5):1357-1368. doi: 10.1002/jmri.26986. Epub 2019 Nov 12. J Magn Reson Imaging. 2020. PMID: 31714648 Free PMC article.
-
Hemodynamic Evaluation of Type B Aortic Dissection Using Compressed Sensing Accelerated 4D Flow MRI.J Magn Reson Imaging. 2023 Jun;57(6):1752-1763. doi: 10.1002/jmri.28432. Epub 2022 Sep 23. J Magn Reson Imaging. 2023. PMID: 36148924 Free PMC article.
-
Noninvasive Morphologic and Hemodynamic Evaluation of Type B Aortic Dissection: State of the Art and Future Perspectives.Radiol Cardiothorac Imaging. 2021 Jun 24;3(3):e200456. doi: 10.1148/ryct.2021200456. eCollection 2021 Jun. Radiol Cardiothorac Imaging. 2021. PMID: 34235440 Free PMC article. Review.
-
In Vitro Studies on Hemodynamics of Type B Aortic Dissection: Accuracy and Reliability.J Endovasc Ther. 2025 Apr;32(2):303-311. doi: 10.1177/15266028231182229. Epub 2023 Jun 21. J Endovasc Ther. 2025. PMID: 37341214 Review.
Cited by
-
Mechanisms of aortic dissection: From pathological changes to experimental and in silico models.Prog Mater Sci. 2025 Apr;150:101363. doi: 10.1016/j.pmatsci.2024.101363. Epub 2024 Sep 12. Prog Mater Sci. 2025. PMID: 39830801 Free PMC article.
-
Questions and Certainty in Diagnosis and Management of Acute Type B Aortic Dissection.Rev Cardiovasc Med. 2025 Feb 20;26(2):26807. doi: 10.31083/RCM26807. eCollection 2025 Feb. Rev Cardiovasc Med. 2025. PMID: 40026512 Free PMC article. Review.
-
False lumen hemodynamics and partial thrombosis in chronic aortic dissection of the descending aorta.Eur Radiol. 2024 Aug;34(8):5190-5200. doi: 10.1007/s00330-023-10513-6. Epub 2024 Jan 6. Eur Radiol. 2024. PMID: 38183450
-
Mitral valve regurgitation assessed by intraventricular CMR 4D-flow: a systematic review on the technological aspects and potential clinical applications.Int J Cardiovasc Imaging. 2023 Oct;39(10):1963-1977. doi: 10.1007/s10554-023-02893-z. Epub 2023 Jun 16. Int J Cardiovasc Imaging. 2023. PMID: 37322317 Free PMC article. Review.
-
Respiratory-resolved five-dimensional flow cardiovascular magnetic resonance : In-vivo validation and respiratory-dependent flow changes in healthy volunteers and patients with congenital heart disease.J Cardiovasc Magn Reson. 2024 Winter;26(2):101077. doi: 10.1016/j.jocmr.2024.101077. Epub 2024 Aug 2. J Cardiovasc Magn Reson. 2024. PMID: 39098573 Free PMC article.
References
-
- Levy D, Goyal A, Grigorova Y, Farci F, Le JK. Aortic Dissection. StatPearls. Treasure Island, FL: StatPearls Publishing LLC; (2022). - PubMed
-
- Rohlffs F, Tsilimparis N, Diener H, Larena-Avellaneda A, Von Kodolitsch Y, Wipper S, et al. Chronic type B aortic dissection: indications and strategies for treatment. J Cardiovasc Surg. (2015) 56:231–8. - PubMed
-
- van Bogerijen GH, Tolenaar JL, Rampoldi V, Moll FL, van Herwaarden JA, Jonker FH, et al. Predictors of aortic growth in uncomplicated type B aortic dissection. J Vasc Surg. (2014) 59:1134–43. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources