

Sex-Specific Associations of Anxiety With Left Ventricular Hypertrophy and Transmural Dispersion of Repolarization in Hypertensive Patients
- PMID: 35757339
- PMCID: PMC9218101
- DOI: 10.3389/fcvm.2022.858097
Sex-Specific Associations of Anxiety With Left Ventricular Hypertrophy and Transmural Dispersion of Repolarization in Hypertensive Patients
Abstract
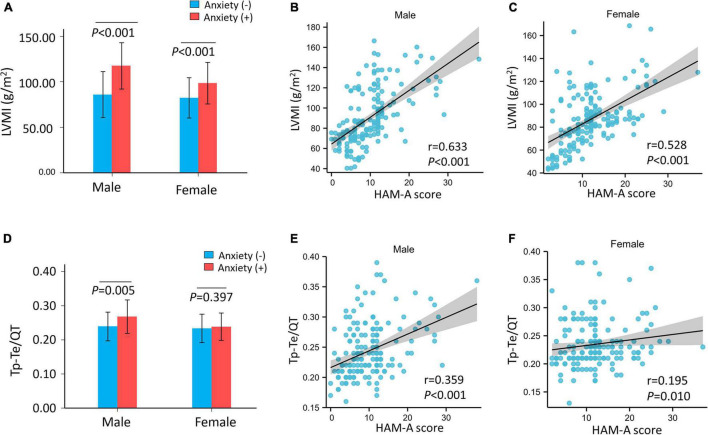
Background: The previous studies have shown that individuals with hypertension and anxiety have a higher mean left ventricular mass index (LVMI) and QTc dispersion. We explored the associations between anxiety and left ventricular hypertrophy (LVH) and between anxiety and transmural dispersion of repolarization (TDR) (as detected by T peak-T end interval/QT interval, Tp-Te/QT ratio) in patients with hypertension.
Methods: A total of 353 patients with uncomplicated hypertension from the Shaanxi Provincial People's Hospital were enrolled between 2017 and 2021. Anxiety was defined as a Hamilton Anxiety Scale (HAM-A) score ≥ 14. Logistic regression models were used to estimate the association between HAM-A and LVH. The association between HAM-A score and Tp-Te/QT was estimated using linear regression.
Results: Participants were divided into two groups based on the presence of anxiety. LVMI was significantly higher in patients with hypertension and anxiety than in those with hypertension without anxiety (no anxiety: 84.36 ± 23.82, anxiety: 105.75 ± 25.45 g/m2, p < 0.001). HAM-A score was positively correlated with LVMI (r = 0.578, p < 0.001) and with Tp-Te/QT (r = 0.252, p < 0.001). Logistic regression models showed that patients with hypertension and anxiety were at higher risk of LVH than were patients with hypertension without anxiety (adjusted OR, 2.44, 95% CI, 1.35-4.43, p = 0.003). The linear regression analysis showed that the HAM-A score was associated with Tp-Te/QT ratio (adjusted β, 0.001, 95% CI, 0.001-0.002, p = 0.013). There was an interaction between sex and anxiety for LVH risk (p for interaction = 0.035) and for increased Tp-Te/QT (p for interaction = 0.014). After stratification by sex, anxiety was associated with increased risk for LVH in men with hypertension (adjusted OR, 5.56, 95% CI, 2.07-14.98, p = 0.001), but not in women (adjusted: OR, 1.44, 95% CI, 0.64-3.26, p = 0.377) with hypertension. The HAM-A score was also positively associated with Tp-Te/QT ratio in male (adjusted β, 0.002, 95% CI, 0.001-0.003, p < 0.001), but not in women (adjusted β, 0.001, 95% CI, -0.0002-0.002, p = 0.165).
Conclusion: Our results indicated that anxiety was associated with LVH and with increased TDR in men with hypertension, but not in women with hypertension.
Keywords: anxiety; hypertension; left ventricular hypertrophy; sex; transmural dispersion of repolarization.
Copyright © 2022 Zhu, Cui, Zhang, Liu, Zhao and Wang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources