Long-term Outcomes of Parenchyma-sparing and Oncologic Resections in Patients With Nonfunctional Pancreatic Neuroendocrine Tumors <3 cm in a Large Multicenter Cohort
- PMID: 35758433
- PMCID: PMC9388557
- DOI: 10.1097/SLA.0000000000005559
Long-term Outcomes of Parenchyma-sparing and Oncologic Resections in Patients With Nonfunctional Pancreatic Neuroendocrine Tumors <3 cm in a Large Multicenter Cohort
Abstract
Introduction: The role of parenchyma-sparing resections (PSR) and lymph node dissection in small (<3 cm) nonfunctional pancreatic neuroendocrine tumors (PNET) is unlikely to be studied in a prospective randomized clinical trial. By combining data from 4 high-volume pancreatic centers we compared postoperative and long-term outcomes of patients who underwent PSR with patients who underwent oncologic resections.
Methods: Retrospective review of prospectively collected clinicopathologic data of patients who underwent pancreatectomy between 2000 and 2021 was collected from 4 high-volume institutions. PSR and lymph node-sparing resections (enucleation and central pancreatectomy) were compared to those who underwent oncologic resections with lymphadenectomy (pancreaticoduodenectomy, distal pancreatectomy). Statistical testing was performed using χ 2 test and t test, survival estimates with Kaplan-Meier method and multivariate analysis using Cox proportional hazard model.
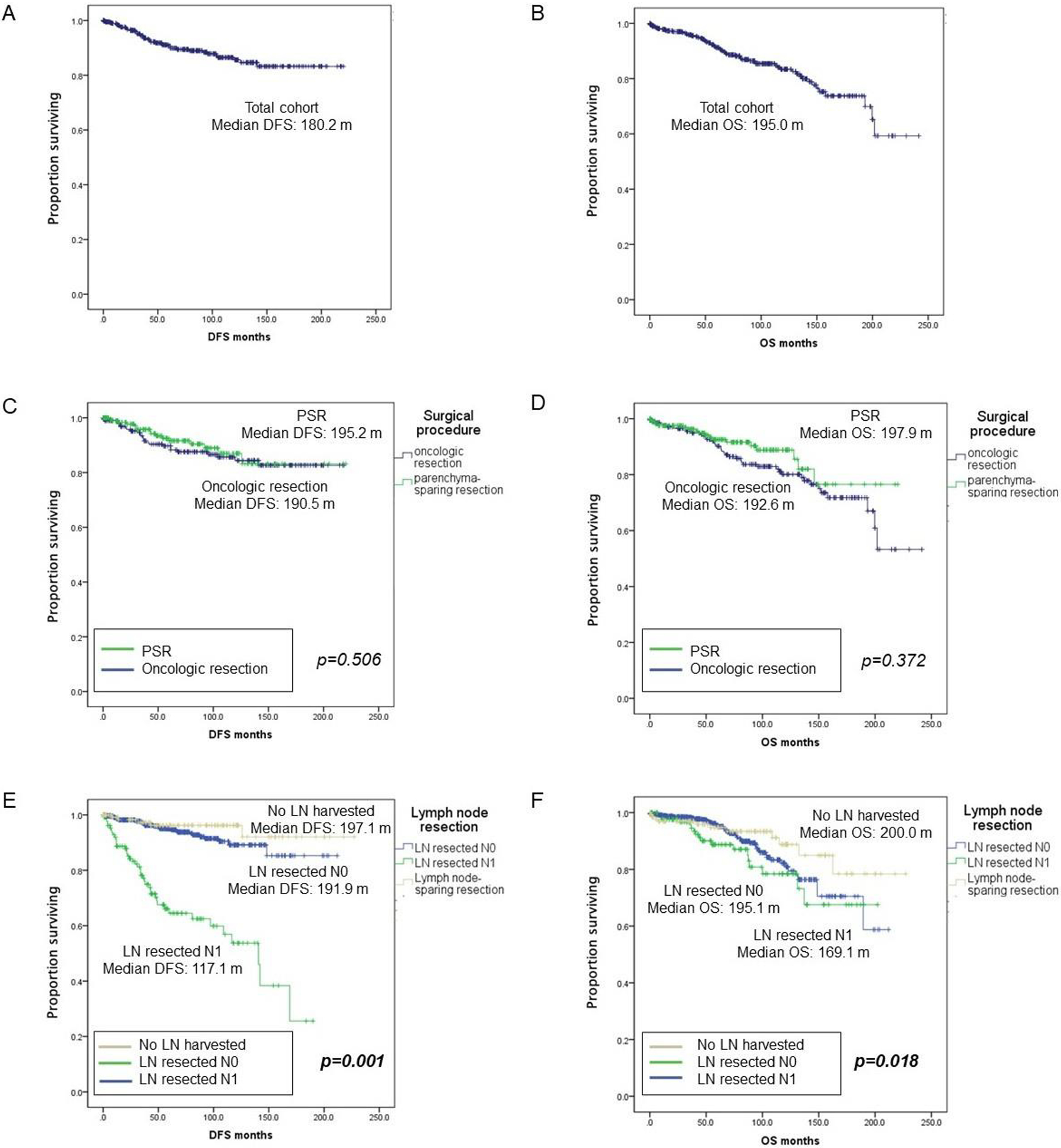
Results: Of 810 patients with small sporadic nonfunctional PNETs, 121 (14.9%) had enucleations, 100 (12.3%) had central pancreatectomies, and 589 (72.7%) patients underwent oncologic resections. The median age was 59 years and 48.2% were female with a median tumor size of 2.5 cm. After case-control matching for tumor size, 221 patients were selected in each group. Patients with PSR were more likely to undergo minimally invasive operations (32.6% vs 13.6%, P <0.001), had less intraoperative blood loss (358 vs 511 ml, P <0.001) and had shorter operative times (180 vs 330 minutes, P <0.001) than patients undergoing oncologic resections. While the mean number of lymph nodes harvested was lower for PSR (n=1.4 vs n=9.9, P <0.001), the mean number of positive lymph nodes was equivalent to oncologic resections (n=1.1 vs n=0.9, P =0.808). Although the rate of all postoperative complications was similar for PSR and oncologic resections (38.5% vs 48.2%, P =0.090), it was higher for central pancreatectomies (38.5% vs 56.6%, P =0.003). Long-term median disease-free survival (190.5 vs 195.2 months, P =0.506) and overall survival (197.9 vs 192.6 months, P =0.372) were comparable. Of the 810 patients 136 (16.7%) had no lymph nodes resected. These patients experienced less blood loss, shorter operations ( P <0.001), and lower postoperative complication rates as compared to patients who had lymphadenectomies (39.7% vs 56.9%, P =0.008). Median disease-free survival (197.1 vs 191.9 months, P =0.837) and overall survival (200 vs 195.1 months, P =0.827) were similar for patients with no lymph nodes resected and patients with negative lymph nodes (N0) after lymphadenectomy.
Conclusion: In small <3 cm nonfunctional PNETs, PSRs and lymph node-sparing resections are associated with lower blood loss, shorter operative times, and lower complication rates when compared to oncologic resections, and have similar long-term oncologic outcomes.
Copyright © 2022 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures