

Intrathecal Morphine and Effect on Opioid Consumption and Functional Recovery after Pancreaticoduodenectomy
- PMID: 35758927
- PMCID: PMC9371061
- DOI: 10.1097/XCS.0000000000000261
Intrathecal Morphine and Effect on Opioid Consumption and Functional Recovery after Pancreaticoduodenectomy
Abstract
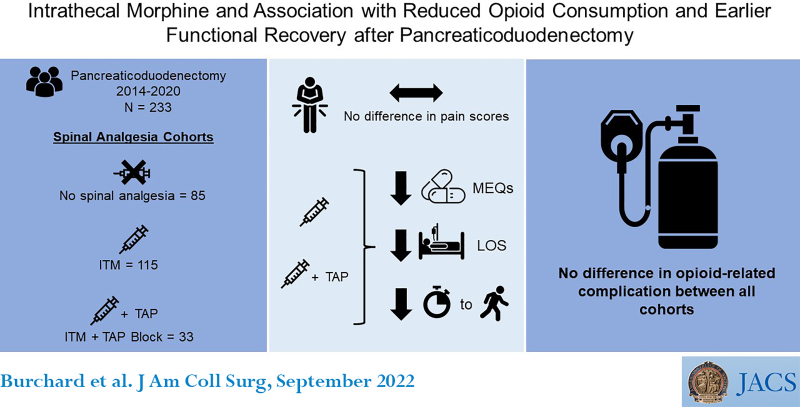
Background: Single-shot intrathecal morphine (ITM) is an effective strategy for postoperative analgesia, but there are limited data on its safety, efficacy, and relationship with functional recovery among patients undergoing pancreaticoduodenectomy.
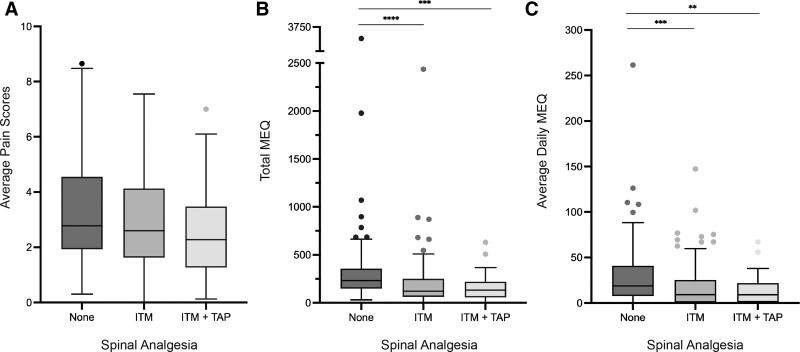
Study design: This was a retrospective review of patients undergoing pancreaticoduodenectomy from 2014 to 2020 as identified by the institutional NSQIP Hepato-pancreato-biliary database. Patients were categorized by having received no spinal analgesia, ITM, or ITM with transversus abdominus plane block (ITM+TAP). The primary outcomes were average daily pain scores from postoperative days (POD) 0 to 3, total morphine equivalents (MEQ) consumed over POD 0 to 3, and average daily inpatient MEQ from POD 4 to discharge. Secondary outcomes included the incidence of opioid related complications, length of stay, and functional recovery.
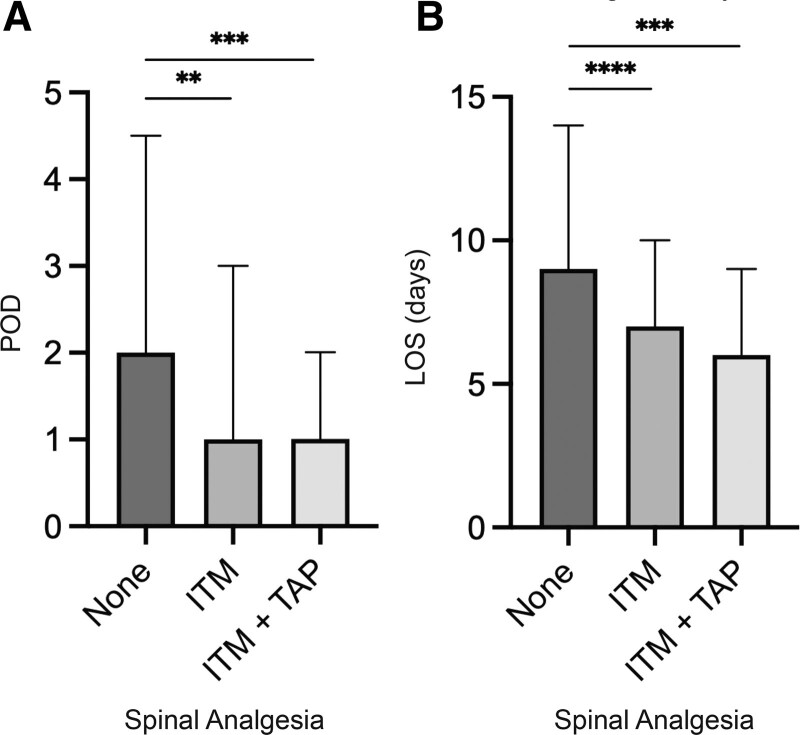
Results: A total of 233 patients with a median age of 67 years were included. Of these, 36.5% received no spinal analgesia, 49.3% received ITM, and 14.2% received ITM+TAP. Average pain scores in POD 0 to 3 were similar by mode of spinal analgesia (none [2.8], ITM [2.6], ITM+TAP [2.3]). Total MEQ consumed from POD 0 to 3 were lower for patients who received ITM (121 mg) and ITM+TAP (132 mg), compared with no spinal analgesia (232 mg) (p < 0.0001). Average daily MEQ consumption from POD 4 to discharge was lower for ITM (18 mg) and ITM+TAP (13.1 mg) cohorts compared with no spinal analgesia (32.9 mg) (p = 0.0016). Days to functional recovery and length of stay were significantly reduced for ITM and ITM+TAP compared with no spinal analgesia. These findings remained consistent through multivariate analysis, and there were no differences in opioid-related complications among cohorts.
Conclusions: ITM was associated with reduced early postoperative and total inpatient opioid utilization, days to functional recovery, and length of stay among patients undergoing pancreaticoduodenectomy. ITM is a safe and effective form of perioperative analgesia that may benefit patients undergoing pancreaticoduodenectomy.
Copyright © 2022 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American College of Surgeons.
Figures
References
-
- Fotiadis RJ, Badvie S, Weston MD, Allen-Mersh TG. Epidural analgesia in gastrointestinal surgery. Br J Surg 2004;91:828–841. - PubMed
-
- McLean SR, von Homeyer P, Cheng A, et al. Assessing the benefits of preoperative thoracic epidural placement for lung transplantation. J Cardiothorac Vasc Anesth 2018;32:2654–2661. - PubMed
-
- Rigg JR, Jamrozik K, Myles PS, et al. MASTER Anaethesia Trial Study Group. Epidural anaesthesia and analgesia and outcome of major surgery: a randomised trial. Lancet 2002;359:1276–1282. - PubMed
-
- Bujedo BM, Santos SG, Azpiazu AU. A review of epidural and intrathecal opioids used in the management of postoperative pain. J Opioid Manag 2012;8:177–192. - PubMed
-
- De Pietri L, Siniscalchi A, Reggiani A, et al. The use of intrathecal morphine for postoperative pain relief after liver resection: a comparison with epidural analgesia. Anesth Analg 2006;102:1157–1163. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
