

Temporal Trends in Antimicrobial Prescribing During Hospitalization for Potential Infection and Sepsis
- PMID: 35759274
- PMCID: PMC9237797
- DOI: 10.1001/jamainternmed.2022.2291
Temporal Trends in Antimicrobial Prescribing During Hospitalization for Potential Infection and Sepsis
Abstract
Importance: Some experts have cautioned that national and health system emphasis on rapid administration of antimicrobials for sepsis may increase overall antimicrobial use even among patients without sepsis.
Objective: To assess whether temporal changes in antimicrobial timing for sepsis are associated with increasing antimicrobial use, days of therapy, or broadness of antimicrobial coverage among all hospitalized patients at risk for sepsis.
Design, setting, and participants: This is an observational cohort study of hospitalized patients at 152 hospitals in 2 health care systems during 2013 to 2018, admitted via the emergency department with 2 or more systemic inflammatory response syndrome (SIRS) criteria. Data analysis was performed from June 10, 2021, to March 22, 2022.
Exposures: Hospital-level temporal trends in time to first antimicrobial administration.
Outcomes: Antimicrobial outcomes included antimicrobial use, days of therapy, and broadness of antibacterial coverage. Clinical outcomes included in-hospital mortality, 30-day mortality, length of hospitalization, and new multidrug-resistant (MDR) organism culture positivity.
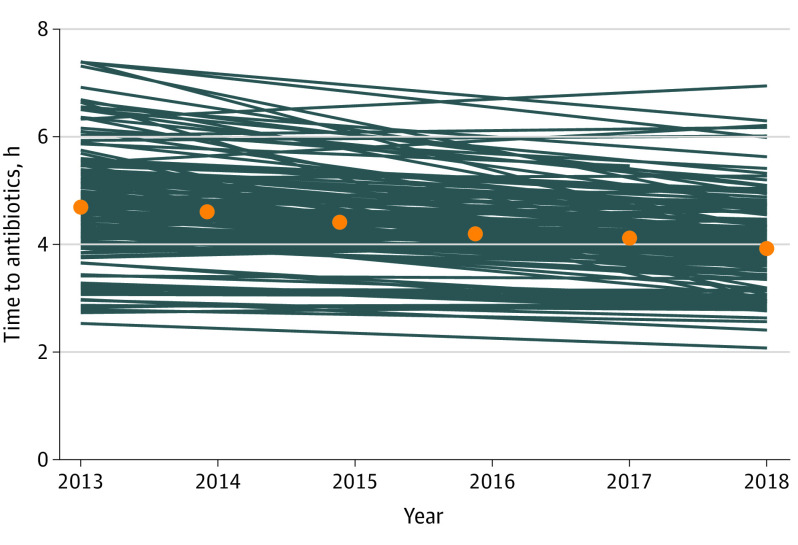
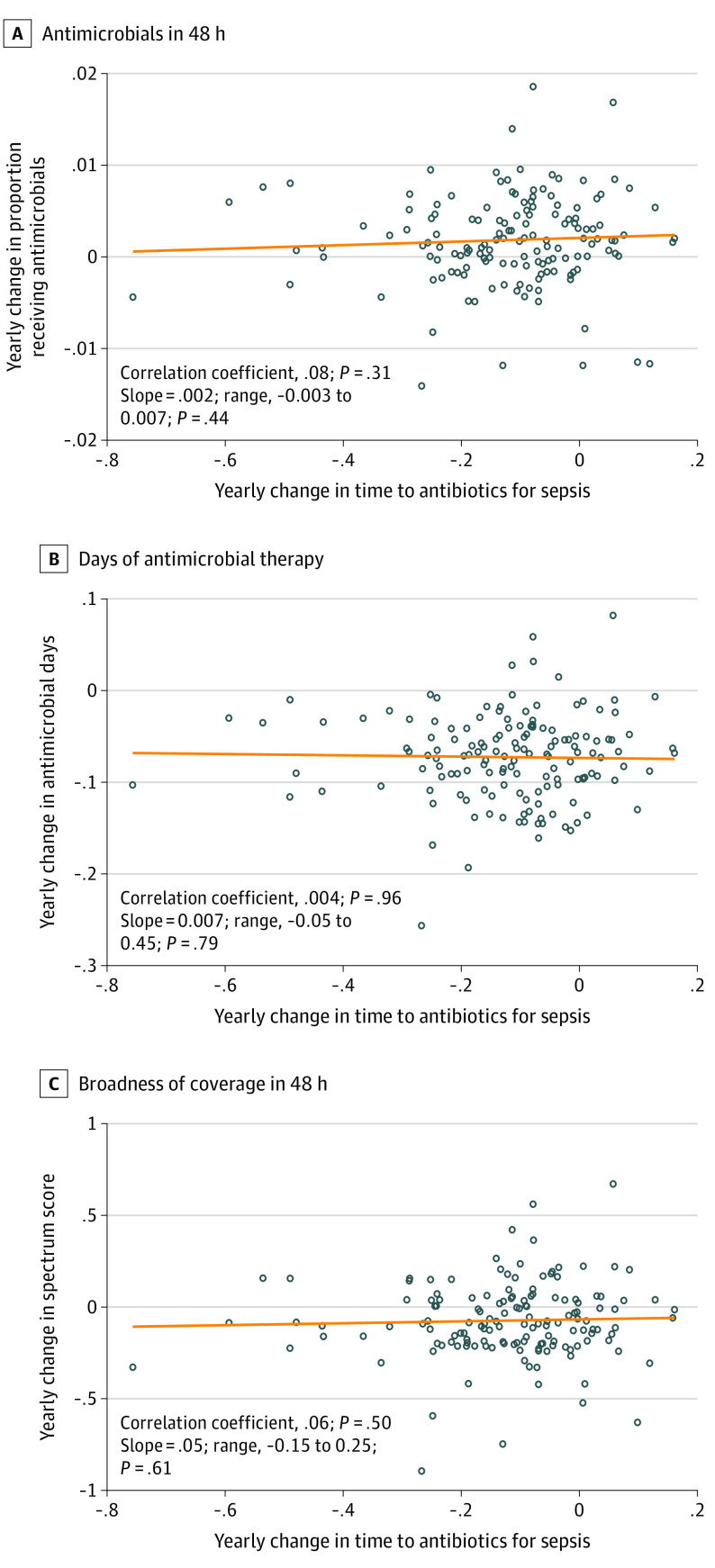
Results: Among 1 559 523 patients admitted to the hospital via the emergency department with 2 or more SIRS criteria (1 269 998 male patients [81.4%]; median [IQR] age, 67 [59-77] years), 273 255 (17.5%) met objective criteria for sepsis. In multivariable models adjusted for patient characteristics, the adjusted median (IQR) time to first antimicrobial administration to patients with sepsis decreased by 37 minutes, from 4.7 (4.1-5.3) hours in 2013 to 3.9 (3.6-4.4) hours in 2018, although the slope of decrease varied across hospitals. During the same period, antimicrobial use within 48 hours, days of antimicrobial therapy, and receipt of broad-spectrum coverage decreased among the broader cohort of patients with SIRS. In-hospital mortality, 30-day mortality, length of hospitalization, new MDR culture positivity, and new MDR blood culture positivity decreased over the study period among both patients with sepsis and those with SIRS. When examining hospital-specific trends, decreases in antimicrobial use, days of therapy, and broadness of antibacterial coverage for patients with SIRS did not differ by hospital antimicrobial timing trend for sepsis. Overall, there was no evidence that accelerating antimicrobial timing for sepsis was associated with increasing antimicrobial use or impaired antimicrobial stewardship.
Conclusions and relevance: In this multihospital cohort study, the time to first antimicrobial for sepsis decreased over time, but this trend was not associated with increasing antimicrobial use, days of therapy, or broadness of antimicrobial coverage among the broader population at-risk for sepsis, which suggests that shortening the time to antibiotics for sepsis is feasible without leading to indiscriminate antimicrobial use.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
