

Association of APOE Genotypes and Chronic Traumatic Encephalopathy
- PMID: 35759276
- PMCID: PMC9237800
- DOI: 10.1001/jamaneurol.2022.1634
Association of APOE Genotypes and Chronic Traumatic Encephalopathy
Erratum in
-
Error in Open Access Status.JAMA Neurol. 2023 Feb 1;80(2):215. doi: 10.1001/jamaneurol.2022.3673. JAMA Neurol. 2023. PMID: 36251311 Free PMC article. No abstract available.
Abstract
Importance: Repetitive head impact (RHI) exposure is the chief risk factor for chronic traumatic encephalopathy (CTE). However, the occurrence and severity of CTE varies widely among those with similar RHI exposure. Limited evidence suggests that the APOEε4 allele may confer risk for CTE, but previous studies were small with limited scope.
Objective: To test the association between APOE genotype and CTE neuropathology and related endophenotypes.
Design, setting, and participants: This cross-sectional genetic association study analyzed brain donors from February 2008 to August 2019 from the Veterans Affairs-Boston University-Concussion Legacy Foundation Brain Bank. All donors had exposure to RHI from contact sports or military service. All eligible donors were included. Analysis took place between June 2020 and April 2022.
Exposures: One or more APOEε4 or APOEε2 alleles.
Main outcomes and measures: CTE neuropathological status, CTE stage (0-IV), semiquantitative phosphorylated tau (p-tau) burden in 11 brain regions (0-3), quantitative p-tau burden in the dorsolateral frontal lobe (log-transformed AT8+ pixel count per mm2), and dementia.
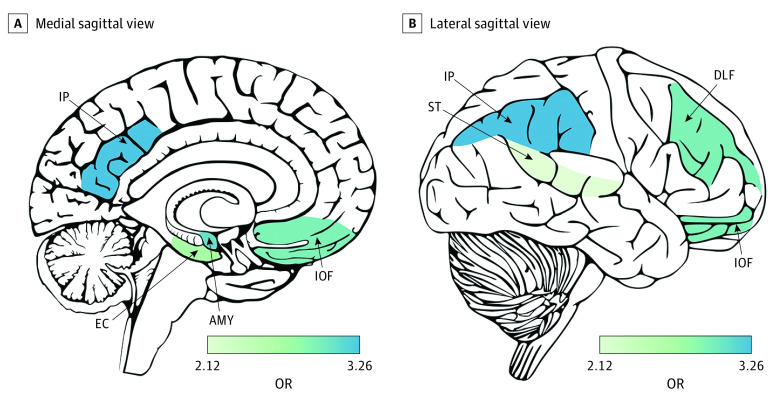
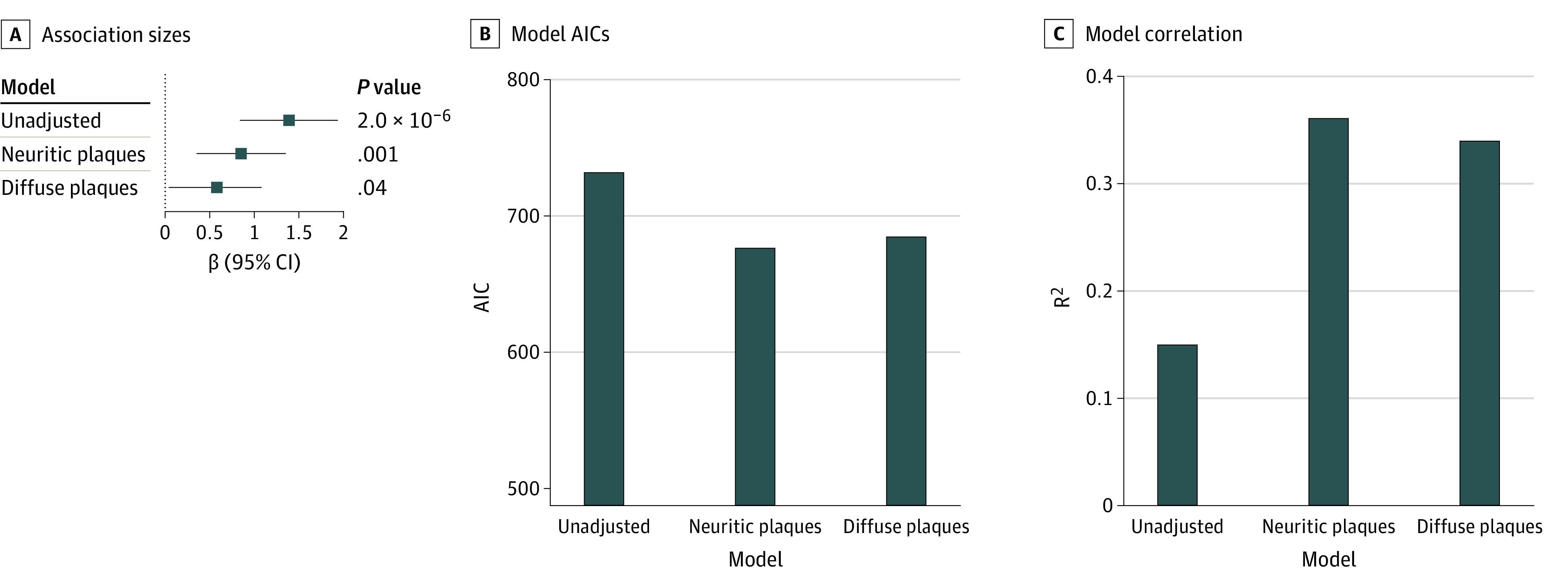
Results: Of 364 consecutive brain donors (100% male; 53 [14.6%] self-identified as Black and 311 [85.4%] as White; median [IQR] age, 65 [47-77] years) 20 years or older, there were 294 individuals with CTE and 70 controls. Among donors older than 65 years, APOEε4 status was significantly associated with CTE stage (odds ratio [OR], 2.34 [95% CI, 1.30-4.20]; false discovery rate [FDR]-corrected P = .01) and quantitative p-tau burden in the dorsolateral frontal lobe (β, 1.39 [95% CI, 0.83-1.94]; FDR-corrected P = 2.37 × 10-5). There was a nonsignificant association between APOEε4 status and dementia (OR, 2.64 [95% CI, 1.06-6.61]; FDR-corrected P = .08). Across 11 brain regions, significant associations were observed for semiquantitative p-tau burden in the frontal and parietal cortices, amygdala, and entorhinal cortex (OR range, 2.45-3.26). Among football players, the APOEε4 association size for CTE stage was similar to playing more than 7 years of football. Associations were significantly larger in the older half of the sample. There was no significant association for CTE status. Association sizes were similar when donors with an Alzheimer disease neuropathological diagnosis were excluded and were reduced but remained significant after adjusting for neuritic and diffuse amyloid plaques. No associations were observed for APOEε2 status. Models were adjusted for age at death and race.
Conclusions and relevance: APOEε4 may confer increased risk for CTE-related neuropathological and clinical outcomes among older individuals with RHI exposure. Further work is required to validate these findings in an independent sample.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
